
Imaging of Diaphragmatic Injury: A Diagnostic Challenge? - PowerPoint PPT Presentation
1 / 53
Title:
Imaging of Diaphragmatic Injury: A Diagnostic Challenge?
Description:
Title: Imaging of Diaphragmatic Injury: A Diagnostic Challenge? Author: naughty Last modified by: user Created Date: 10/12/2004 11:59:32 AM Document presentation format – PowerPoint PPT presentation
Number of Views:75
Avg rating:3.0/5.0
Title: Imaging of Diaphragmatic Injury: A Diagnostic Challenge?
1
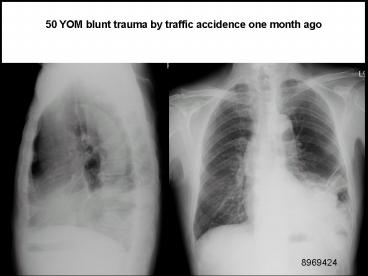
50 YOM blunt trauma by traffic accidence one
month ago
8969424
2
(No Transcript)
3
(No Transcript)
4
(No Transcript)
5
Unilateral Diaphragmatic Elevation
- 1.Subpulmonic pleural effusion
- dome of pseudodiaphragm migrates toward
the costophrenic angle and flattens - 2.Altered pulmonary volume
- (a)Atelectasis
- associated pulmonary density
- (b)Postoperative lobectomy / pneumonectomy
- rib defects, metallic sutures
- (c)Hypoplastic lung
- small hemithorax (more often on the
right), crowding of ribs, mediastinal shift,
absent / small pulmonary artery, frequently
associated with dextrocardia anomalous
pulmonary venous return
6
- 3.Phrenic nerve paralysis
- (a)Primary lung tumor
- (b)Malignant mediastinal tumor
- (c)Iatrogenic
- (d)Idiopathic
- paradoxic motion on fluoroscopy
(patient in lateral position sniffing) - 4.Abdominal disease
- (a)Subphrenic abscess history of surgery,
accompanied by pleural effusion - (b)Distended stomach / colon
- (c)Interposition of colon
- (d)Liver mass (tumor, echinococcal cyst,
abscess) - 5.Diaphragmatic hernia
- 6.Eventration of diaphragm
- 7.Traumatic rupture of diaphragm
- Associated with rib fractures, pulmonary
contusion, hemothorax - 8.Diaphragmatic tumor
- Mesothelioma, fibroma, lipoma, lymphoma,
metastases
7
Imaging of Diaphragmatic Injury A Diagnostic
Challenge?
- S. Iochum, T Ludig, F Walter, H Sebbag, G
Grosdidier, and AG BlumRadioGraphics 2002 22
103S - ??? ???
8
Anatomy
- Central tendon
- Crus
- Hiatus3
- Celiac trunk
- Inf. Phrenic n.
9
(No Transcript)
10
(No Transcript)
11
(No Transcript)
12
- type 1 configuration(48). The anterior component
is concave posteriorly and continuous with the
anterolateral diaphragmatic fibers (arrowheads). - type 2 configuration(28). The anterior muscle
fibers appear to be oriented at an angle in
relation to the lateral fibers with midline
discontinuity (arrowhead). - type 3 configuration(11). The anterior muscle
fibers lie anteriorly within a single plane.
13
- CT scan shows that the diaphragm is not well
demonstrated due to the proximity of the liver,
which has the same attenuation. Note the
diaphragmatic slips that attach to the ribs
(arrowheads). - The coronal and sagittal planes are better than
axial planes in analysis of the diaphragm.
14
Mechanisms of Injuries
- Traumatic diaphragmatic injuries occur in 0.8
Recommended
CrystalGraphics Presentations





























