
CONCLUSIONS PowerPoint PPT Presentation
1 / 1
Title: CONCLUSIONS
1
fMRI activation patterns elicited by saccadic
tasks in prediagnostic Huntington disease Jason
Rupp, David Kareken, Mario Dzemidzic, Veronique
Bragulat, Joanne Wojcieszek, Tanya Blekher,
Tatiana Foroud
IndianaCTSI ACCELERATING CLINICAL AND
TRANSLATIONAL RESEARCH
INTRODUCTION
RESULTS
Huntington disease (HD) is an autosomal dominant,
neurodegenerative disease caused by the expansion
of a poly-CAG tract in the huntingtin gene (Table
1). HD is characterized by motor, mood, and
cognitive abnormalities. We previously showed
that prediagnostic HD subjects exhibited deficits
in oculomotor tasks (Blekher et al, 2006). To
extend this work, we developed an event-driven
fMRI paradigm to examine cortical and subcortical
activity associated with the conscious, cognitive
preparation to inhibit reflexive gaze in an
anti-saccade (AS task.
Representative traces from a PS and an AS trial
are shown in Figure 2, and a performance summary
is shown in Figure 3. Correct ASgtcorrect PS
evoked more activation in both CAG- and preHD.
Areas of activation in CAG- included the
frontoparietal network and the basal ganglia
(Figure 4, panels a and b), while preHD
activations were confined primarily to the
frontal lobe and the basal ganglia (Figure 4,
panels c and d). When comparing this pattern
between groups directly, this greater activation
in the parietal areas of CAG- could only be
observed in a small number of voxels at a low
p-value of 0.01. There was significantly more
activation in the head of the right caudate and
the right frontal operculum (FO)/insula in preHD
than CAG- (Figure 4, e). In preHD, correct
ASgtincorrect AS showed activation in the basal
ganglia (Figure 5), while there were no such
areas in CAG. In CAG- (Figure 6, panels a and
b) incorrect ASgtcorrect AS elicited more
activation in the anterior cingulate, caudate,
FO/insula, medial frontal cortex, precuneus, and
cuneus, none of which were observed in preHD. The
between-groups comparison (Figure 6, panels c and
d) revealed greater activation in the anterior
cingulate and basal ganglia in CAG- than in
preHD. The opposite contrast (preHDgtCAG-) did
not yield any significant regions.
METHODS
Thirty-two subjects completed the imaging
protocol. Twelve were CAG- and 19 were CAG.
Using the UHDRS, 7 CAG subjects were deemed with
99 confidence to have a diagnosis of HD, and
these subjects were excluded from further
analysis. The other 12 CAG subjects were
considered prediagnostic (preHD). The CAG- and
preHD groups did not differ significantly for
age, gender, or education (pgt0.2). The
event-driven protocol comprised 4 runs of 32
pseudo-randomized trials of either pro-saccade
(PS) or AS trials (Figure 1). Imaging data were
collected on a Siemens 3T TIM-Trio scanner and
analyzed using SPM5. Event onset was timed with
the display of the instruction prompt. A
factorial random effects model with group (CAG-
or preHD) by trial outcome (correct PS, correct
AS, or incorrect AS) was employed. Eye
movement data were collected during imaging.
Using an interactive program written in MATLAB,
each saccade was classified as correct or
incorrect. Trials with blinks during instruction
period were removed from analysis. Performance
was computed as follows for each individual for
the PS and AS trials proportion correct
correct trials / (correct incorrect trials).
Group effects were tested using analysis of
covariance (ANCOVA) with education, age, and
gender as covariates.
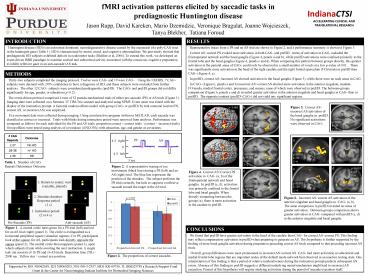
Figure 1. A central circle turns green for a PS
trial (left) and red for an AS trial (right)
(panel 1). The circle is extinguished as a
horizontal peripheral square (stimulus) appears.
For PS, participants look at the square for AS,
participants look directly opposite the square
(panel 2). The central circle then reappears
(panel 3), upon which subjects fixate while
awaiting the next instruction. A single task run
consists of 16 PS and 16 AS trials. Repetition
time (TR) 2000 ms. Yellow star correct eye
position.
CONCLUSIONS
We found that preHD have greater activation in
the head of the caudate than CAG- for correct
ASgtcorrect PS. This finding may reflect
compensatory activation in preHD when preparing
to generate an AS. This hypothesis is further
supported by the finding of more basal ganglia
activation during preparation preceding correct
AS trials compared to that preceding incorrect AS
trials. Overall, group differences were most
pronounced in incorrect ASgtcorrect AS. CAG- had
more activation in subcortical and medial frontal
lobe regions that are important nodes of the
default mode network best observed in an inactive
resting state. One interpretation of this finding
is that a period of relative inattentiveness
during the instruction prompt predicts subsequent
AS errors. Absence of this finding in preHD
suggests a different underlying neural mechanism
might lead to incorrect AS execution. Pursuit of
this hypothesis will require studying activation
during the period of saccade execution itself.
Figure 3. The proportions of correct saccades.
Supported by R01 NS042659, R21 NS060205,
N01-NS-3-2357, MO1 RR-00750, TL1RR025759 a
Research Support Fund Grant the Center for
Neuroimaging/Indiana Institute for Biomedical
Imaging Sciences
Recommended
