
Intraocular Suturing of the Dislocated IOL to the Ciliary Sulcus PowerPoint PPT Presentation
Title: Intraocular Suturing of the Dislocated IOL to the Ciliary Sulcus
1
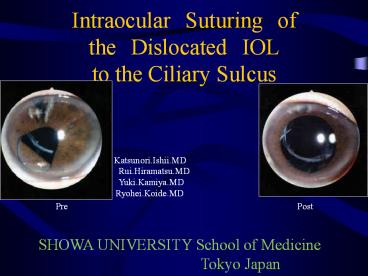
Intraocular Suturing of the Dislocated IOL to
the Ciliary Sulcus
Katsunori.Ishii.MD Rui.Hiramatsu.MD
Yuki.Kamiya.MD Ryohei.Koide.MD
Pre
Post
SHOWA UNIVERSITY School of Medicine
Tokyo Japan
2
PURPOSE
- To describe a technique of intraocular
double-knot suturing for scleral fixation of in
the bag dislocated intraocular lens - METHOD
- We are using two 20-gauge corneal tunnels with
20-gauge CCC forceps - We should move the haptic of dislocated
intraocular lens on the iris
3
STEP 1 (Below the haptic)
Scleral flap, two 20 gauge corneal tunnels are
created. Viscoelastic needle is inserted below
the dislocated haptic, and docked with double
long 10-0 straight needle through the lens
capsule.
4
STEP 2 (Above the haptic)
A 20G CCC forceps is inserted above the haptic,
used to grasp the 10-0 suture on the optics
softly and then 10-0 suture in a U shape is then
guided corneal tunnel.
5
STEP 3 (First ligature)
We selected a 10-0 suture in a U shape through
both corneal tunnels. The selected 10-0 suture is
rotated twice clockwise on a straight needle.
Both straight needles are slowly pulled back, and
the first ligature is made on the haptics in the
eye.
6
STEP 4 (Above the haptic again)
Following the first ligature, a 20G CCC forceps
is inserted above the haptic again, used to grasp
the 10-0 suture on the optics softly and then
10-0 suture in a U shape is then guided corneal
tunnel.
7
STEP 5 (Second ligature)
Following the first ligature, we selected a 10-0
suture through both corneal tunnels. The
selected 10-0 suture is rotated once
counter-clockwise a straight needle. Both
straight needles are slowly pulled back, and the
second ligature is made on the haptics in the eye.
8
STEP 6 (Cutting a 10-0)
Following the Second ligature, we cut a 10-0
suture of double knot out of the cornea.
9
STEP 7 (Intraocular suturing)
A long needle is once again inserted into the eye
though corneal tunnel a 25G needle is threaded
through the corneoscleral flap and docked inside
the eye, the loop is in position below the iris,
and intraocular suturing is complete.
10
CASE
age Post- VA Pre-ope complications Percent decrease in endothelial cells operation (min)
76 10/100 Dementia 6(2907?2740) 32
58 1/100 Post-RD Not measured 59
63 20/20 Not measured 30
37 20/20 1(2725?2710) 55
48 20/20 Post-RD 4(2660?2558) 46
63 20/20 3(2652?2584) 37
28 20/20 Post-RD Not measured 55
11
DISCUSSION
- In the bag IOL dislocation is uncommon
complication - This intraocular suturing is simple and strong
ligature, in addition, the site was small. - This procedure reduced operating time and
required no vitrectomy, because of the limited
impact on the capsule. - We experienced the postoperative temporary high
intraocular pressure, because of residual
viscoelastic substance. - There were few previous cases in which this
procedure was used , and careful follow-up is
required in the future.
12
REFERENCE
- 1)Dimitri T.Azar,William F.WileyDouble-knot
transscleral suture fixiation technique for
displaced interaocular lensesAm J
Ophthalmol128644-646.1999 - 2)Koh HJ,Kim CY,Lim SJ et al Scleral fixation
technique using 2 corneal tunnels for a
dislocated intraocular lens. J Cataract Refract
Surg 26 1439-1441,2000 - 3)Kwok AKH, Cheng ACK, Lam DSC Surgical
technique for transcleral fixation of a
dislocated posterior chamber intraocular lens .Am
J Ophthalmol 132 406-408.2001 - 4)Kokame GT, Atebara NH, Bennett MD Modified
technique of haptic externalization for scleral
fixation of dislocated posterior chamber lens
implants. Am J Ophthalmol 131129-130.2001 - 5)Hanemoto T, Ideta H,Kawasaki T Dislocated
intraocular lens fixation using intraocular
cowhitch knot.Am J Ophthalmol 131 265-267,2001
Recommended
