
Definitive Radiation Therapy for Squamous Cell Carcinoma of the Soft Palate
1 / 1
Title:
Definitive Radiation Therapy for Squamous Cell Carcinoma of the Soft Palate
Description:
The National Cancer Institute's Surveillance Epidemiology and End Results (SEER) ... Bhishamjit S. Chera M.D., Robert Amdur M.D., Russell Hinerman M.D., *Douglas ... –
Number of Views:193
Avg rating:3.0/5.0
Title: Definitive Radiation Therapy for Squamous Cell Carcinoma of the Soft Palate
1
Definitive Radiation Therapy for Squamous Cell
Carcinoma of the Soft Palate
Bhishamjit S. Chera M.D., Robert Amdur M.D.,
Russell Hinerman M.D., Douglas Villaret M.D.,
John Werning M.D., and William Mendenhall
M.D. Department of Radiation Oncology at the
University of Florida, Gainesville, FL And
Department of Otolaryngology
Table 1 Patient Characteristics
Introduction
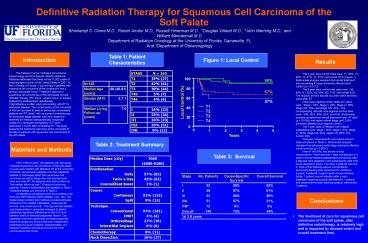
Figure 1 Local Control
Results
The National Cancer Institutes Surveillance
Epidemiology and End Results (SEER) statistical
database estimates that there will be 11,800
cases of oropharyngeal cancer in the United
States in 2007. At the University of Florida, 1
out of every 4 patients with squamous cell
carcinoma of the oropharynx has a primary
soft-palate tumor. Treatment options for squamous
cell carcinomas of the soft palate include
radiation therapy (RT) alone, surgery alone, or
surgery followed by postoperative radiotherapy.
Chemotherapy is often used concurrently with RT
for advanced disease. The current policy at the
University of Florida has been to treat all
previously unirradiated patients with RT alone,
with concurrent chemotherapy for advanced-stage
disease, and neck dissection reserved for
residual radiographically suspicious nodes on a
computed tomography (CT) scan performed 1 month
after completing RT. This study presents the
treatment outcomes at the University of Florida
for patients with squamous cell carcinomas of the
soft palate.
The 5-year local control rates were T1, 90
T2, 90 T3, 67 T4, 57 and overall, 81
(Figure 1). Multivariate analysis revealed that
overall treatment time exceeding 47 days
adversely affected local control (p
0.0172). The 5-year neck control rate rates
were N0, 90 N1, 82 N2, 68 N3, 71, and
overall 82. The majority of neck failures
occurred within the first 2 years after
RT. Initial local-regional control rates at 5
years, were Stage I, 84 Stage II, 85 Stage
III, 66 Stage IVA, 59 and Stage IVB, 43.
The corresponding ultimate local-regional control
rates were 89, 88, 96, 63, and 43.
Multivariate analysis revealed that overall
treatment time gt47 days (p 0.0190) and higher
overall stage (p0.0158) adversely affected
local-regional control. The 5-year rates of
freedom from distant metastases were stage I,
95 stage II, 97 stage III, 100 stage IVA,
93 stage IVB, 69 and overall, 94.
Five-year cause-specific and overall survival
rates are shown in Table 3. Multivariate
analysis revealed that advanced nodal stage
adversely affected overall survival (p lt
0.0001). Nine of 145 (6) had severe or fatal
complications. There was only 1 fatal
complication in a patient who developed
postoperative pneumonia after a planned neck
dissection and subsequently died from acute
respiratory failure. The other 8 patients had one
or more of the following severe complications
permanent feeding tube placement for nutritional
support, 4 patients surgical repair of
orocutaneous fistula, 1 patient wound infection
after a neck dissection requiring surgical
debridement, 1 patient and osteoradionecrosis
requiring surgical intervention, 3 patients.
Table 2 Treatment Summary
Materials and Methods
Table 3 Survival
From 1963 to 2004, 145 patients with previously
untreated squamous cell carcinomas of the soft
palate or uvula were treated with definitive RT
at the University of Florida. We excluded
patients who had metastatic disease or
histologies other than squamous cell carcinoma as
well as those who had received prior head and
neck RT. No patients were lost to follow-up. The
median follow-up was 7.6 years for surviving
patients. Patient characteristics are depicted in
Table 1. Treatment details can be found in Table
2. All statistical calculations were
accomplished with SAS and JMP software (SAS
Institute, Cary, NC). The Kaplan-Meier product
limit method provided estimates of freedom from
distant metastasis, cause-specific survival, and
overall survival. The log-rank test statistic
was implemented in univariate analyses to detect
statistically significant differences at the 0.05
level between strata of selected prognostic
factors. Cox regression was then performed on
these prognostic factors to isolate any factors
that were independent predictors of a given
endpoint implementation of a backward selection
procedure insured the most parsimonious final
model.
Conclusions
- The likelihood of cure for squamous cell
carcinoma of the soft palate, after definitive
radiotherapy, is relatively high and is impacted
by disease extent and overall treatment time.
Recommended
CrystalGraphics Presentations





























