
Mortality in People with Diabetes Causes of Death - PowerPoint PPT Presentation
1 / 31
Title:
Mortality in People with Diabetes Causes of Death
Description:
Age-Specific Prevalence of the metabolic syndrome among 8814 US adults aged at ... A positive history for percutaneous transluminal coronary angioplasty (PTCA) ... – PowerPoint PPT presentation
Number of Views:46
Avg rating:3.0/5.0
Title: Mortality in People with Diabetes Causes of Death
1
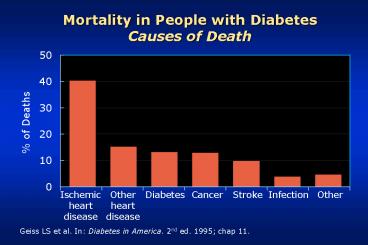
Mortality in People with DiabetesCauses of Death
of Deaths
Ischemicheartdisease
Otherheartdisease
Diabetes
Cancer
Stroke
Infection
Other
Geiss LS et al. In Diabetes in America. 2nd ed.
1995 chap 11.
2
(No Transcript)
3
(No Transcript)
4
Variation in mortality for CHD in USA Gu K, et
al. JAMA, 2811291-1297,1999
Mortalità per cardiopatia coronarica ()
Non diabetici
Diabetici
5
Age-Specific Prevalence of the metabolic syndrome
among 8814 US adults aged at least 20 years, by
sex, National Health and Nutrition Examination
Survey III, 1988-1994
Prevalence
Age (years)
6
Prevalence of insulin resistance with associated
metabolic disorders
100
80
60
Prevalence of HOMA insulinresistance ()
40
20
0
0
1
2
3
4
Number of metabolic disorders
Metabolic disorders glucose intolerance,
dyslipidaemia, hyperuricaemia and/or
hypertensionplt0.001 for differences in
prevalence rates across categories
7
(No Transcript)
8
(No Transcript)
9
(No Transcript)
10
ATP III Framingham Risk Scoring
Nota Le stime del rischio sono state derivate
dallesperienza del Framingham Heart Study, con
una popolazione di razza predominante Caucasica
11
Prevalence of asyntomatic CHD
12
Incidenza di infarto fatale e non fatale in
relazione a eventuale pregresso infarto
East-West Study Follow-up a 7 anni
50
45.0
40
plt0.001
30
Incidenza durante il follow-up ()
20.2
18.8
20
plt0.001
10
3.5
0
(n69)
(n1304)
(n169)
(n890)
Eventi per100 persone-anno
3.0
0.5
7.8
3.2
Haffner SM et al. N Engl J Med 1998339229-234.
13
(No Transcript)
14
CAPRIE steering Committee. A randomised, blinded.
Trial of clopidogrel versus aspirin in patients
at risk of ischaemic events Lancet 1996
3481329-1339
Aronow WS, Ahn C. Prevalence of coexistence of
coronary artery disease, peripheral arterial
disease, and atherothrombotic brain infarction in
men and women lt62 years of age. Am J Cardiol
1994 74 64-65
15
(No Transcript)
16
Incidenza di ictus fatale e non fatale in
relazione a eventuale pregresso infarto
Follow-up a 7 anni East-West Study
25
19.5
20
plt0.001
15
Incidenza durante il follow-up ()
10.3
10
7.2
p0.01
5
1.9
0
(n69)
(n1304)
(n169)
(n890)
Eventi per100 persone-anno
1.2
0.3
3.4
1.6
17
High cardiovascular disease mortality in subjects
with visual impairment caused by diabetic
retinopathy (Rajala U et al, Diabetes Care 23
957-961,2000)
Cumulative survival after 4 years
18
Complicanze CHD4.280 visite a diabetici
19
(No Transcript)
20
The Metabolic Syndrome NCEP classification
- Abdominal Obesity waist gt102 cm in M and gt88 cm
in F - Triglycerides ?150 mg/dl
- HDLlt40 mg/dl in M and lt50 mg/dl in F
- PA ?130/85 mm Hg
- FPG ?110 mg/dl
(National Cholesterol Education Program-NCEP-III
Report. JAMA 16 285 (5) 2001).
21
The Aims
- How each component of the Metabolic Syndrome
aggregate in Type 2 diabetes? - Do components of the Metabolic Syndrome
significantly associate with prevalent coronary
artery disease in Type 2 diabetes?
22
DAI STUDY The Metabolic Syndrome (1)
23
DAI STUDY The Metabolic Syndrome (2)
Percentage of patients
24
DAI STUDY The Metabolic Syndrome (3). Prevalence
of the components segregating with type 2 diabetes
Percentage
Number of Metabolic Abnormalities
25
DAI STUDY The Metabolic Syndrome (4). Prevalence
of a single component
Percentage
Metabolic Abnormalities
26
The presence of CHD was assessed as follows
- A positive history for hospital admission for
either an acute myocardial infarction (AMI) or an
episode of angina - A positive 12-lead ECG for prior acute myocardial
infarction or angina coded using the Minnesota
coding system (criteria I 1-3, IV 1-3, V 1-2, and
VII 1) - A positive history for coronary artery by-pass
graft (CABG) - A positive history for percutaneous transluminal
coronary angioplasty (PTCA).
27
(No Transcript)
28
(No Transcript)
29
(No Transcript)
30
Logistic analysis of the variables associated to
CHD in type 2 diabetic patients in Italy
Odd ratio
31
Steno 2 Conclusions
Taken together, these data suggest that a
long-term, targeted, intensive intervention
involving multiple risk factors reduces the risk
of both cardiovascular and microvascular events
by about 50 per cent among patients with type 2
diabetes and microalbuminuria
NEJM 2003 348 383-93
Recommended
CrystalGraphics Presentations





























