
ARTS II: Patient Flow PowerPoint PPT Presentation
1 / 32
Title: ARTS II: Patient Flow
1
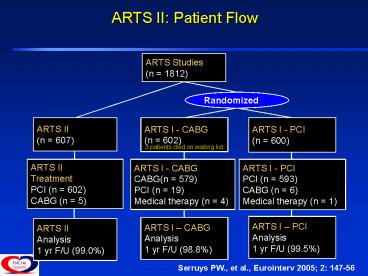
ARTS II Patient Flow
ARTS Studies (n 1812)
Randomized
ARTS II (n 607)
ARTS I - CABG (n 602)
ARTS I - PCI (n 600)
3 patients died on waiting list
ARTS II Treatment PCI (n 602) CABG (n 5)
ARTS I - CABG CABG(n 579) PCI (n 19) Medical
therapy (n 4)
ARTS I - PCI PCI (n 593) CABG (n 6) Medical
therapy (n 1)
ARTS I PCI Analysis 1 yr F/U (99.5)
ARTS I CABG Analysis 1 yr F/U (98.8)
ARTS II Analysis 1 yr F/U (99.0)
Serruys PW., et al., Eurointerv 2005 2 147-56
2
ARTS II - Baseline Demographics
26 (5)
67
74
Figures in Orange indicate statistical difference
(95 CI) between ARTS II and ARTS I groups
3
ARTS II - Lesion Characteristics
4
ARTS II - Procedural Characteristics
ARTS I (PCI) N600 pts N1606 les.
ARTS I (CABG) N605 pts N1638 les.
ARTS II N607 pts N2160 les.
Lesions,
2.8
2.8
3.6
Stented les. / anast. seg.,
2.5
2.6
3.2
Stents,
2.8
-
3.7
Direct stenting,
3
-
35
Max. inflation pressure, atm
14.6
-
16.4
Total stent length, mm
48
-
73
8-165
-
12-253
(range)
Gp IIb/IIIa inhibitor use,
-
-
33
Use of arterial conduit,
-
93
-
Duration of procedure, mins
99
193
85
Hospital stay, days
3.9
9.6
3.4
5
ARTS II
ARTS II 3-Year Follow-up
607 patients
18 death
1,080 Days Follow-up
589 Alive
414 Seen at outpatient clinic with ECG
175 Not seen at outpatient clinic
Lost to FUP 2/175
Death gt1080days 2/175
Withdrawal 3/175
- Phone contact patient 140/168
- By GP 9/168
- By relative 2/168
- Other 17/168
ECG obtained 132/168
No ECG obtained 36/168
ECG obtained by center Died at 1087 and
1116 days
Serruys PW., et al., ACC 2007 Oral Presentation.
6
ARTS II
ARTS II Mortality Through 3 Years
97.0
96.0
95.6
P (log rank) 0.20 between ARTS II and ARTS I-CABG
- ARTS II - ARTS I CABG - ARTS I PCI
P (log rank) 0.33 between ARTS II and ARTS I-PCI
0
6
12
18
24
30
36
Time (Months)
Serruys PW., et al., ACC 2007 Oral Presentation.
7
ARTS II
ARTS II Death, Cerebrovascular Accidents, and
MIs Through 3 Years
92.0
89.1
87.2
P (log rank) 0.07 between ARTS II and ARTS I-CABG
- ARTS II - ARTS I CABG - ARTS I PCI
P (log rank) 0.004 between ARTS II and ARTS I-PCI
0
6
12
18
24
30
36
Time (Months)
Serruys PW., et al., ACC 2007 Oral Presentation.
8
ARTS II
ARTS II ST Through 3 Years
Re-adjudication according to Dublin definitions
- Definite (angiography pathological
confirmation) - Definite Probable (MI in stent
area) - Definite, probable and possible (any
unexplained death)
10
9
8
7
6.4
6
5.3
of Patients
5
4
3.3
3
2
1
0
0
180
360
540
720
900
1080
30
Serruys PW., et al., ACC 2007 Oral Presentation.
9
ARTS II
ARTS II Reintervention Through 3 Years
P (log rank) lt0.001
93.4
85.5
- ARTS II - ARTS I CABG - ARTS I PCI
73.3
P (log rank) lt0.001 between ARTS II and ARTS I-PCI
0
6
12
18
24
30
36
Time (Months)
Serruys PW., et al., ACC 2007 Oral Presentation.
10
ARTS II
ARTS II Diabetic Population
ARTS I (PCI) 112-patients 309-lesions
ARTS I (CABG) 96-patients 290-lesions
ARTS II 159-patients 568-lesions
Patient characteristics (main differences)
73
79
76
Male ()
63
63
64
Age (years)
64
56
80
Hypertension
74
74
55
49
Hypercholesterolemia
Lesion characteristics
6
6
15
Lesion length gt 20mm ()
13
15
33
Calcified lesion ()
7
7
17
Type C lesion
3.6
2.9
3.0
of lesions gt 50DS
2.5
2.8
3.2
of treated lesions
Serruys PW., et al., ACC 2007 Oral Presentation.
11
ARTS II
ARTS II Diabetic Population (3 Years)
- Hierarchical MACCE ARTS II ARTS I (CABG)
ARTS I(PCI) up to 3 years N159
N96 N112
8 (7.1)
8 (5.0)
5 (5.2)
Death
5 (5.2)
5 (4.5)
4 (2.5)
Stroke
3 (1.9)
3 (3.1)
8 (7.1)
MI
0 (0.0)
11 (9.8)
6 (3.8)
CABG
21 (18.8)
23 (14.5)
4 (4.2)
Repeat PCI
17 (17.7)
53 (47.3)
44 (27.7)
MACCE
-
8 (7.1)
2 (1.3)
Stent thrombosis
Without death Without death and stroke
Without death, stroke and MI Without death,
stroke, MI or CABG
Figures in Orange indicate statistical difference
(95 CI) between ARTS II and ARTS I groups
Serruys PW., et al., ACC 2007 Oral Presentation.
12
ARTS II
ARTS II Summary
- In ARTS II the risk profile of the patients (DM,
HTN, ?lipids, vessels and lesions) has
increased with respect to ARTS I however, the
clinical success rate (in-hospital) is excellent
without procedural death. - The SAT rate per patient at 30 days is 1.0 with
the CYPHER stent (ARTS II), which is lower than
the 2.8 with the CROWN and CrossFlex LC
stents. The cumulative rate of definite
stent thrombosis at 3 years is 3.3. - Despite the higher risk profile, the overall
MACCE rate at 3 years is lower in ARTS II than in
the ARTS I-PCI and not significantly different
from ARTS I-CABG arms.
Serruys PW., et al., ACC 2007 Oral Presentation.
13
ARTS II
ARTS II Summary
- However, the reintervention rate of the ARTS
I-CABG is still significantly lower than in ARTS
II Total population p lt 0.001 - In conclusion the overall MACCE
- rate of ARTS II at 3 year is non-inferior to
ARTS I-CABG
Serruys PW., et al., ACC 2007 Oral Presentation.
14
6 TOPICS OF THIS PRESENTATION
1. Historical review of randomized trials on PCI
vs. CABG
2. ARTS 1 5-year FU
3. ARTS 2 3 year FU
4. WHATS THE SYNTAX SCORE ?
15
SYNTAX Score
SYNTAX score
- Goal SYNTAX score to provide guidance on optimal
revascularization strategies for patients with
high risk lesions
EUROINTERV 2006
16
(No Transcript)
17
(No Transcript)
18
(No Transcript)
19
(No Transcript)
20
(No Transcript)
21
6 TOPICS OF THIS PRESENTATION
1. Historical review of randomized trials on PCI
vs. CABG
2. ARTS 1 5-year FU
3. ARTS 2 3 year FU
4. WHATS THE SYNTAX SCORE ?
5. SYNTAX SCORE IN ARTS 2 TRIAL
22
ARTS 2
23
(No Transcript)
24
(No Transcript)
25
(No Transcript)
26
(No Transcript)
27
26
28
6 TOPICS OF THIS PRESENTATION
1. Historical review of randomized trials on PCI
vs. CABG
2. ARTS 1 5-year FU
3. ARTS 2 3 year FU
4. WHATS THE SYNTAX SCORE ?
5. SYNTAX SCORE IN ARTS 2 TRIAL
6. SYNTAX, FREEDOM - SUMMARY
29
SYNTAX Study Design
All Patients with 3VD/LM
Heart Team (surgeon and interventionalist)
amenable for one treatment approach
amenable for both treatments options
Randomized Arm N1500 (11)
Two Registry Arms
CABG 2750 captured (750 followed)
PCI All captured and followed
vs
TAXUS
CABG
- reasonable doubt
- follow-up 30d, 6m, 1-5 yrs
- Goal to define the most appropriate treatment
through randomized trial methods
- consensus exists that only one treatment option
(CABG vs PCI) is appropriate - Goal to profile larger pool of non randomizable
patients and their subsequent outcomes
30
FREEDOM Study Design
Diabetes Mellitus with 2-3VD
surgeon and interventionalist
31
FREEDOM
- RANDOMIZED 766p
- INCOR 62p - 8
- 32p CABG 2 DEATHS
- 30p PCI
- 16 TAXUS 14 CYPHER
- 1 DEATH (TX)
- 1 CABG (TX)
32
(No Transcript)
33
A RESPOSTA É SIM, MAS NÃO EM TODOS OS PACIENTES
MULTIARTERIAIS.NOS PACIENTES COM CARACTERÍSTICAS
ANGIOGRÁFICAS MAIS COMPLEXAS A CIRURGIA AINDA É A
MELHOR OPÇÃO. DEVEMOS AGUARDAR FREEDOM E SYNTAX
PARA AS CONCLUSÕES DEFINITIVAS.
Recommended
