
Diabetes Mellitus Type 2 PowerPoint PPT Presentation
1 / 56
Title: Diabetes Mellitus Type 2
1
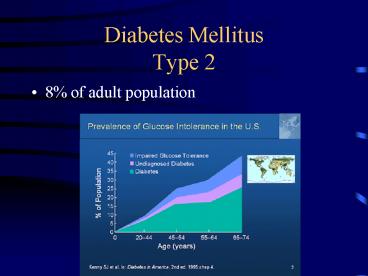
Diabetes MellitusType 2
- 8 of adult population
2
Presentation
- Fatigue
- Weight loss
- The three Ps
- Blurred vision
- Infections
- Muscle cramps
- Poor healing
3
(No Transcript)
4
Diagnosis of Diabetes
Also a random glucose gt200 mg/dL symptoms of
hyperglycemia
5
Metabolic syndrome(a.k.a. Syndrome X)
- ? Definition (ATP III vs WHO)
- ? Name cardiometabolic risk
- Associated with an increased risk of diabetes,
cardiovascular and overall mortality - Abdominal obesity
- Dyslipidemia (low HDL, hypertriglyceridemia)
- Impaired glucose metabolism (Fasting glucose
gt100mg/dl) - Hypertension
6
Metabolic Syndrome
- WHO
- FPG gt 110 mg/dl 2 of the following
- Waist/hip ratio gt.9 or abdominal Girth gt 37
inches - HDL lt 35mg/dl Triglyceridesgt150mg/dl
- BP gt 140/90
- ATP III
- 3 of the following
- Abdominal girth gt40 inches in men
gt35 inches in women - HDL lt 40 mg/dl in men lt 50 mg/dl in women
- Triglycerides gt150 mg/dl
- BPgt 130/85
- FPG gt 100 mg/dl
7
Screening for Diabetes
8
Classifications
- Type1
- lt10 of Diabetics
- Normal to underweight
- Age of onset lt40, peaking at 14
- abrupt onset of symptoms
- Pathogenesis is insulin deficiency (B-cell
destruction) - Diabetic ketoacidosis
- Type 2
- gt90 of Diabetics
- Obese patients
- Age of onsetgt40
- Gradual onset of symptoms
- pathogenesis is insulin resistance others
- Non-ketotic hyperosmolar syndrome
9
(No Transcript)
10
Treatment
- Patient Education
- Lifestyle modification
- exercise
- risk reduction
- diet
- disease monitoring
- Pre-prandial vs post-prandial testing
- Recognition and treatment of hypoglycemia
11
Diabetic Diet
- Individualized, there is no standard ADA diet.
- Limit total (20-30) and saturated fats (lt10)
- Limit carbohydrates to achieve desired weight
loss (250-500 cal below calculated needs) - The amount and not the source is important
- Calorie exchanges to tailor diet to medications
- Limit protein if nephropathy exits
12
Hypertension in Diabetes
- ACE inhibitor
- Primary prevention of diabetic nephropathy
- Secondary prevention
- decrease proteinuria
- slows the decline of the GFR
- May improve insulin sensitivity
- Cardiovascular benefits (CAPP, HOPE, ABCD)
- Need to watch for the development of hyperkalemia
associated with hyporenin hypoaldosteronism
13
Hypertension in Diabetes
- Angiotensin II receptor blockers
- NEJM Sept.2001
- Renal protective, with some evidence of
cardiovascular benefits (LIFE, diabetes subgroup
analysis) - May be appropriate first line agent in type II
- Calcium channel blockers
- non-dihydropyridines (verapamil, diltiazem)
- prevention of diabetic nephropathy?
- neutral effect on glucose tolerance and lipids
14
Hypertension in Diabetes
- Despite concerns regarding diuretics and
B-blockers propensity to worsen glucose control
and adversely effect lipids, they have been
shown to be safe and effective in controlling BP
in diabetics. - B-blockers can also mask the adrenergic symptoms
of hypoglycemia - What is your blood pressure goal?
15
130/80
16
Tight Blood Pressure Control in Diabetes
- UKPDS- tight control defined as lt150/85
- Actual average blood pressures were 144/82 vs
154/87 - Associated with lower stroke, retinopathy and
Diabetic related deaths - HOT study-diastolic BP goal of 80
- Resulted in lower cardiovascular deaths and
events compared with goal of 90. - ABCD trial-128/75 achieved BP
- Tight BP control associated with lower overall
mortality 5.5 vs 10.7 for moderate control
(137/81)
17
Tight control of Blood Pressure vs Tight Control
of Blood Sugar
18
Model of Multihormonal Regulationof Glucose
Homeostasis
- Incretin
- Mimetics
- GLP-1 analogs
- Exenatide
Brain
Liver
Metformin
Stomach
PostprandialGlucagon
Rate ofglucoseappearance
Alpha- glucosidase inhibitors
Plasma Glucose
Rate ofglucosedisappearance
Insulin
- Amylin analogs
- Pramlintide
TZDs
Pancreas
Tissues
Insulin Secretagogues
19
Oral Sulfonylureas
- First generation (chlorpropamide, tolazamide,
tolbutamide) - Second generation
- Glyburide 2.5-20 mg a day
- Gypizide 5-40mg a day
- Glimepiride 1-8 mg a day
- Stimulates pancreatic insulin secretion
- side effects weight gain, hypoglycemia, Sudden
death?
20
Biguanides
- Metformin (Glucophage)
- Recommended as initial treatment of type 2
diabetes - 500 mg BID to start, max dose 2500 mg a day
- mechanism of action
- decrease hepatic gluconeogenesis
- improve peripheral insulin resistance
- side effects
- GI diarrhea, cramps, nausea
- Sustained release agents decrease G.I. Side
effects - lactic acidosis
21
Biguanides
- Lactic acidosis
- Less common than phenformin
- Usually associated with CHF, renal
insufficiency, liver disease, hypoxia, Etoh
abuse, IV contrast dye. - Black box warning avoid in CHF and CKD
(creatininegt1.5 in men, 1.4 in women) - Doesnt cause weight gain
- hypoglycemia is rare
22
Thiazolidinediones
- Trogltazone (Rezulin)
- Pulled from the market March , 2000 due to
hepatotoxicity - Rosiglitazone (Avandia)
- 4-8 mg/day (daily or BID)
- Pioglitazone (Actos)
- 15-45 mg/day
23
- Work by improving peripheral insulin sensitivity
- can be used as mono-therapy or with other oral
agents. (caution with insulin) - Maintains beta cell function
- Pioglitizone with lipid benefits (raise HDL,
lower triglycerides) - Side effects include
- weight gain (12bs)
- possible liver toxicity
- increase plasma volume (caution with CHF)
- ? Increase cardiovascular risk in Rosiglitizone
24
Meglitinides
- Repaglinide (Prandin)
- Nateglinide (Starlix)
- Stimulates 1st phase pancreatic insulin secretion
(rapid and short acting) - short half-life
- Take 15-30 minute prior to eating
- no insulin stimulation between mealsless weight
gain
25
Alpha-glucosidase Inhibitor
- Acarbose (Precose), miglitol (Glyset)
- delays carbohydrate digestion
- reduces postprandial hyperglycemia
- 25-100 md T.I.D.
- Side effects
- abdominal pain, bloating, flatulence
26
GLP-1 Modes of Action in Humans
- Stimulates glucose-dependent insulin secretion
- Suppresses glucagon secretion
- Slows gastric emptying
GLP-1 is secreted from the L-cells in the
intestine
- Reduces food intake
- Improves insulin sensitivity
Long term effectsdemonstrated in animals
This in turn
- Increases beta-cell mass and maintains
beta-cell efficiency
Drucker DJ. Curr Pharm Des 2001
71399-1412Drucker DJ. Mol Endocrinol 2003
17161-171
27
Incretin mimetic
- Byetta (exenatide)
- Subcutaneous injection BID
- Mechanism of action
- Stimulates the GLP-1 receptors
- Stimulates insulin release in response to meals
- Inhibits release of glucagon
- Slows GI absorption, reduces food intake
- Improves insulin sensitivity, maintains beta-cell
function - Side effects
- Nausea
- Pancreatitis
28
- Januvia (sitagliptin)
- Prolongs the action of Incretins
- Inhibits DPP-4 enzyme
- 100 mg once a day dosing
- Requires renal dosing-50mg if GRFlt60, 25 mg if
lt30 - Well tolerated
- No weight gain, hypoglycemia or GI disturbance
29
Mechanism of Action of Sitagliptin (Januvia)
Glucose dependent
? Insulin (GLP-1andGIP)
? Glucose uptake by peripheral tissue
Ingestion of food
Pancreas
Release of active incretins GLP-1 and GIP
Beta cells Alpha cells
? Blood glucose in fasting and postprandial states
GI tract
X
Glucose- dependent
DPP-4 enzyme
Sitagliptin (DPP-4 inhibitor)
? Hepatic glucose production
? Glucagon (GLP-1)
Inactive GLP-1
Inactive GIP
- Incretin hormones GLP-1 and GIP are released by
the intestine throughout the day, and their
levels ? in response to a meal.
In healthy subjects, sitagliptin did not lower
blood glucose or cause hypoglycemia
GLP-1glucagon-like peptide-1 GIPglucose-depende
nt insulinotropic polypeptide.
30
Amylin Analogue
- Symlin (pramlintide)
- Synthetic analogue of beta cell hormone
- Reduces postprandial glucagon secretion
- Increases satiety, slows gastic emptying
- Containdicated in patients with gastroparesis
- Dosed q AC
- Can cause hypoglycemia
31
Insulin
Short acting (regular, Lispo) Intermediate (NPH,
lente) mixture 70/30, 75/25 Long acting
(ultalente, lantus)
32
Approximate Pharmacokinetic Profiles of Human
Insulin and Insulin Analogues
Hirsch, I. B. N Engl J Med 2005352174-183
33
New Insulins
- Lispro/Aspart/Apidra
- Shorter onset and duration of action than R
- less hypoglycemia
- treat postprandial hyperglycemia
- Glargine (Lantus)/Determir (Levemir)
- steady duration of action for 24 hours
- peakless release
- less hypoglycemia
34
Insulin regimens
35
Standard Regimen
36
Poor mans Insulin Pump
37
Long term complications
- Retinopathy
- Neuropathy
- Nephropathy
- Arteriosclerosis
38
Retinopathy
- Diabetics are also at increased risk of cataracts
39
Non-proliferative Retinopathy
40
- Also called background retinopathy
- can develop in as early as 3-5 years
- see microaneurysms, dot-blot hemorrhages, hard
exudates - usually does not lead to blindness
41
Proliferative Retinopathy
42
- Occurs in Response to retinal ischemia (cotton
wool exudates) - neo-vascularization
- vitreous hemorrhages can result
- Fibro-proliferative changes result in retinal
traction and detachment if the hemorrhage is not
treated.
43
Treatment
- Prevention
- Primary and secondary
- strict glycemic control (Hgb A1clt7.0)
- strict blood pressure control (? additional
benefit from ACE inhibitors) - Secondary
- avoid strenuous activities to prevent hemorrhage
- photocoagulation
- vitrectomy
- Required after a hemorrhage to avoid permanent
blindness
44
Nephropathy
45
- Develops in 35-45 of all diabetics (type 1 and
2) - Hypertension and poor glycemic control will
accelerate the process - Progression from microalbuminuria to end stage
renal failure
46
Microalbuminuria
- 30-300mg of albumin per 24 hours
- random albumin-to-creatinine ratio preferred
diagnostic test - can occur as early as 5 years after the onset of
Diabetes - also a risk factor for cardiovascular disease and
early mortality from cardiovascular disease
47
Proteinuria
- Greater than 300mg/day of albumin
- detectable on a dipstick urinalysis
- renal function is typically preserved (may
actually have glomerular hyper-filtration and
super-normal creatinine clearance) - usually associated with the onset of hypertension
in type 1 (type 2 patients frequently have
essential hypertension in addition to their
diabetes)
48
Nephrotic Syndrome
- gt3.5 grams of protein /24 hours
- associated with falling GFR
- development of peripheral edema
- usually seen 5-10 years after the development of
proteinuria
49
Treatment of nephropathy
- Primary Prevention
- strict glycemic control (Hgb A1clt7.0)
- Diabetes Control and Complications Trial
- Ace inhibitors, ARBs
- Secondary Prevention
- strict glycemic control (Hgb A1clt7.0)
- Ace inhibitors, ARBs
- strict blood pressure control 130/80
- 125/75 if renal insufficiency
50
Neuropathy
- Peripheral sensory-motor neuropathy
- symptoms
- symmetrical stocking glove distribution
- numbness, paresthesia, dysesthesia
- early signs
- decrease sensation (mono-filament test)
- decrease Achilles reflex
- decrease vibratory sensation
51
Treatments
- Prevention (primary and secondary)
- strict glycemic control (HgbA1clt7.0)
- Pain medications
- Antidepressants
- TCAs, duloxetine (Cymbalta)
- seizure medications
- carbamazepoine, phenytoin, gabapentin, pregabalin
(Lyrica) - topical preparations
- capsacin
52
Neuropathy
- Motor
- cranial neuropathy (III,IV,VI)
- peripheral neuropathy
- Median nerve
- foot drop
53
Autonomic Neuropathy
- Gastroparesis
- Diarrhea/constipation
- Orthostasis/resting tachycardia
- Impotency/retrograde ejaculation
54
Arthrosclerosis
- Cerebral Vascular Disease
- Coronary Vascular Disease
- Peripheral Vascular Disease
- Impaired Lipid Profile
- Elevated Triglycerides
- Low HDL
- Small Dense athrogenic LDL particles
55
Recommendations
- Strict glycemic control (ADA)
- HgbA1clt7.0 (AACE recommends lt6.5)
- Pre-prandial glucose 90-130mg/dl
- 1-2hr post-prandial sugars lt180mg/dl
- Requires motivated and compliant patients
- Strict blood pressure control
- lt130/80
- Use ACE inhibitors/ARBs 1st line
- Annual Eye examinations
- Annual micro-albumin checks
56
Recommendations
- Tight lipid management
- LDLlt100 mg/dl
- Patients age gt40 use statins to lower LDL by
30-40 - Goal lt 70mg/dl Prove It trial
- Triglycerideslt150 mg/dl
- HDLgt40 mg/dl in men and gt50 mg/dl in women
- Foot checks at each office visit
- Aspirin therapy recommended for all diabetics
Recommended
