
Comparison of Laparoscopic Hepatectomy and Living Donor Hepatectomy' PowerPoint PPT Presentation
1 / 1
Title: Comparison of Laparoscopic Hepatectomy and Living Donor Hepatectomy'
1
Comparison of Laparoscopic Hepatectomy and
Living Donor Hepatectomy.
Dr Ravishankar K Diddapur. MBBS, MS(Gen-Surg),
FRCS(Glasg), FRCS(GenSurg-Transplant),
FAMS(Singapore), Hesperis Diploma in
Transplantation(European College of
Transplantation-ECOT). Consultant Surgeon, HPB
surgery Liver Transplantation Gleneagles
Hospital, Singapore.
RESULTS
INTRODUCTION Laparoscopic surgery has
revolutionized modern medicine. A minimally
invasive approach to abdominal and thoracic
surgery has resulted in the reduction of patient
pain and postoperative intestinal dysfunction,
while minimizing lengths of hospital stay and
enabling patients to return more rapidly to their
daily activities than does open surgery.
Laparoscopic surgery has established itself as
standard of care in many procedures as
cholecystectomy, fundoplication, bariatric
surgery. Liver resection represents the next
frontier in laparoscopic surgery.
AIM To present the early experience with
laparoscopic liver resection in Singapore.
METHODS We performed laparoscopic left lateral
segmentectomy in two patients in year 2005 and
comparison of open Donor left lateral
segmentectomy ( segment 2 and 3) as a part of
living related transplant is presented. Patient
1 56 year Chinese lady with background history
of Hepatitis B carrier state, Hypertension and
hyperlipidemia. She presented with segment 2/3
liver cyst on screening ultrasound for hepatitis
B. Subsequent imaging showed progressive
enlargement of the cyst. CT scan prior to
resection showed a 56 x 34mm hypo dense lesion in
segment 2/3. The tumor markers were normal so
were the liver function tests. Post-operative
histology showed a choledochalcyst Patient 2
39 year old Malay lady presented with right
upper quadrant pains and obstructive jaundice.
Ultrasound of Hepatobiliary system showed thick
walled gall bladder with multiple stones and an
indeterminate 1.5 cm nodule in segment 3. Further
evaluation with Triphasic CT scan and MRI
suggested 1 x1.5, hypervascular lesion in segment
3 with indeterminate characteristics. The tumor
markers were normal. She initially underwent ERCP
, sphincterotomy and extraction of ductal stones.
Surgical options were discussed with her after
the liver functions settled. Post operative
histology showed a liver focal nodular
hyperplasia and chronic cholecystitis. Patient 3
( used in this presentation for a comparative
control) 35 years old chinese male, liver donor
for his son with biliary atresia and end stage
liver disease. He underwent open donor segment
2/3 liver resection following evaluation with the
protocol for live donor liver transplantation.
Evaluation Both patients ( patient 1 and 2 )
underwent standard preoperative evaluation for a
major laparoscopic procedure under general
anesthesia. Operative Procedure Patient and
instrument positioning The patient is positioned
on the operating table in a supine position with
both arms by the side and the surgeon stands on
the left side of the patient. Monitors are placed
on either side of the patient. The first
assistant stands on the opposite side and the
second assistant variably on right or left
side. The trocars are placed as shown in figure
1. Pneumoperitoneum To minimize a risk of air
embolism, insufflation pressure should be kept as
low as possible (preferably below 12 mmHg). The
patient should also be closely monitored for
vital parameters and end-tidal CO2 level
throughout the entire operation. Argon plasma
coagulator was not used to minimise risk of air
embolism. Preparation and resection Cholecystecto
my is performed using the standard techniques,
the cystic duct is used for methylene blue test
or intraoperative cholangiogram to check for bile
leaks. The falciform ligament is transected,
using the endostapler (ATW 45 Vascular stapler,
Ethicon) and the stump is grasped for retraction.
Next the left triangular ligament is divided to
mobilize the left lateral segments.
Laparoscopic ultrasound is then performed to
confirm the findings. The portal pedicle is
slinged with a vascular tape for a possible
Pringles maneuver. The resection line is marked
with diathermy. Hepatic transection is performed
with a harmonic scalpel (Ultracision, Ethicon),
diathermy . Portal pedicle and left hepatic vein
are divided with application of a linear stapler
(Ethicon). Bleeding is controlled with
application of diathermy, clips, harmonic
scalpel. At the end of resection diluted
methylene blue is instilled through the cystic
duct using a cholangiocatheter and absence of
bile leak is confirmed. If any bile leak is
encountered a, it is controlled with sutures. The
cystic duct is clipped and a lavage performed
after hemostasis. Fibrin glue (Floseal Baxter)
is applied to the raw surface of the liver. The
specimens ( liver and gall bladder) are retrieved
in a endopouch. The umbilical wound is enlarged
vertically to 5- 7 cm to facilitate the specimen
extraction. The ports are removed and all wounds
10mm or more are closed with PDS and finally the
skin is closed.
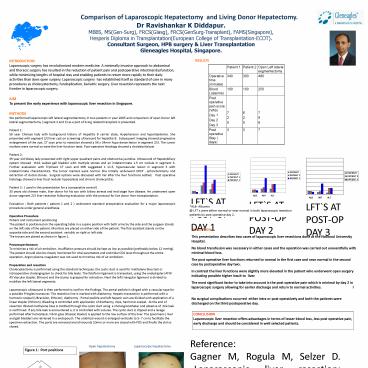
LFTS AT POST-OP DAY 1
LFTS AT POST-OP DAY 2
LFTS AT POST-OP DAY 3
ALB- Albumin _at_ LFTs were either normal or near
normal in both laparoscopic resection patients by
post operative day 2.
DISCUSSION This presentation describes two cases
of laparoscopic liver resections done at the
National University Hospital. No blood
transfusion was necessary in either cases and the
operation was carried out uneventfully with
minimal blood loss. The post operative liver
functions returned to normal in the first case
and near normal in the second case by
postoperative day two. In contrast the liver
functions were slightly more elevated in the
patient who underwent open surgery indicating
possible higher insult to liver. The most
significant factor to take into account is the
post operative pain which is minimal by day 2 in
laparoscopic surgery allowing for earlier
discharge and return to normal activities. I
No surgical complications occurred either
intra or post operatively and both the patients
were discharged on the third postoperative day.
CONCLUSION Laparoscopic liver resection offers
advantages in terms of lesser blood loss, less
post operative pain, early discharge and should
be considered in well selected patients.
Reference Gagner M, Rogula M, Selzer D.
Laparoscopic liver resection benefits and
controversies. Surg Clin North Am. 2004
Apr84(2)451-62. NB This work was done by the
author while he was at NUH, Singapore.
Open hepatectomy
Laparoscopic hepatectomy
Figure 1 Port positions
Recommended
