
Femoropopliteal PTA PowerPoint PPT Presentation
1 / 19
Title: Femoropopliteal PTA
1
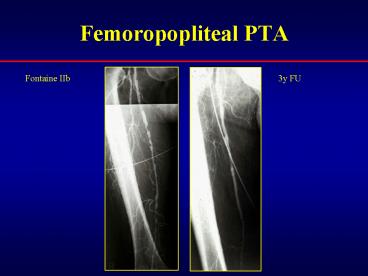
Femoropopliteal PTA
3y FU
Fontaine IIb
2
IndicationsTASC J Vasc Surg 2000
- Type A Endovascular therapy (ET) is the
treatment of choice - Type B ET is more commonly used but more
evidence is needed to make any firm
recommendations - Type C Surgery is more commonly used but more
evidence is needed to make any firm
recommendations - Type D Surgery is the treatment of choice
3
IndicationsTASC J Vasc Surg 2000
- Type A
- Single stenosis up to 3 cm in length
- Type B
- Single stenosis or occlusion up to 10 cm long
- Heavily calcified stenosis up to 3 cm long
- Multiple stenoses or occlusions each less than 3
cm long - Single or multiple lesions to improve inflow for
distal surgical bypass
Type A
Type B
4
IndicationsTASC J Vasc Surg 2000
- Type C
- Single stenosis or occlusion
- gt 10 cm long
- Multiple stenoses or occlusions, each 3-5 cm
- Type D
- Complete CFA and/or SFA occlusion
- Complete popliteal and proximal trifurcation
occlusion
Type D
Type C
5
PTA ResultsTASC J Vasc Surg 2000
6
Stents
Primary indication bail out
7
Stents
- Complications
- thrombosis
- intimal hyperplasia
1y FU
Lysis
48hr
Stent
8
Stents ResultsTASC J Vasc Surg 2000
9
PTA/Stents claudicationMuradin et al,
Radiology 2001
PTA Stent Stenosis patency range patency ra
nge 1y 77 78-80 75 73-79 2y 66
63-71 67 65-71 3y 61 55-68 66
64-70 4y 57 54-63 -- -- 5y 55
52-62 -- -- Occlusion 1y 65 55-71 73
69-75 2y 54 45-61 66 61-68 3y 48
40-55 64 59-67 4y 44 36-53 -- -- 5y
42 33-51 -- --
10
PTA/Stents critical ischemiaMuradin et al,
Radiology 2001
PTA Stent Stenosis patency range patency ra
nge 1y 60 46-63 74 68-80 2y 49
35-54 66 59-72 3y 43 30-51 65
58-71 4y 40 26-46 -- -- 5y 38
24-44 -- -- Occlusion 1y 47 41-51 73
68-75 2y 36 28-41 65 60-68 3y 30
20-37 63 58-68 4y 27 16-34 -- -- 5y
25 13-32 -- --
11
PTA and Stent for Treatment of Femoropopliteal
artery disease Meta-AnalysisMuradin et al,
Radiology 2001
- Conclusion
- PTA and stent implantation for claudication and
stenosis yield similar long-term patency rates - for more severe femoropopliteal artery disease
(occlusion, CLI) the results of stent
implantation seem more favorable
12
PTA vs Palmaz stent in femoropopliteal arteries.
Randomized trialCejna et al JVIR 2001
- Inclusion criteria
- claudication or CLI
- sfa or proximal pa
- up to 3 lesions (stenosis/ occlusion)
- lt 5 cm
- gt 1 patent run-off vessel
- intention to treat
- Endpoints of the study
- primary endpoint 12 months primary patency
rate - secondary endpoints primary technical success
rate complication rate secondary patency
rate
13
PTA vs Palmaz stent trialPrimary technical
success rate
Limbs (n 154)
Primary PTA (n 77)
Primary stent (n 77)
succesfull (n65) 84.4
succesfull (n76) 98.7
p0,02
secondary stent implantation (n 10) 13.0
residualstenosis (n 1) 1.3
14
PTA versus Palmaz stent -primary angiographic/
US patency
63
15
PTA versus Palmaz stent -primary hemodynamic/
clinical patency
77 72
16
PTA versus Palmaz stent -secondary angiographic/
US patency
86 79
17
PTA vs Palmaz stent trialCejna et al JVIR 2001
- Conclusion
- Primary stent placement significantly decreased
technical failure rate (p lt 0.02) - Primary stent placement did not improve mid-term
angiographic and clinical/hemodynamic success
rate - Secondary stent placement
- is indicated if PTA fails
- reveals results similar to PTA
18
Complications
n all major surgery death PTA Becker 4662 10.0
5.6 2.5 0.2 Capek 152 5.5 Matsi
106 10.5 4.0 2.0 Matsi 295 10.5
(CLI) 0.5 (CI) Johnston
236 6.3 Hunink 106 2.4 Gardiner 3.0 TAS
C 1241 4.3 Stents Strecker
80 8.8 Cejna 141 2.6 Henry
126 14 Lammer 74 2.1 TASC 585 7.3
19
PTA/Stents in femoropopliteal arteries
- Conclusion
- short lesions (lt 3cm, type A) are ideal
indications for endovascular treatment - in claudicants patency rates are similar for PTA
and stents (gt 60 at 3y) - in more severe disease (type B and C, CLI)
stents or stentgrafts may be more favorable
(patency of 73-75 at 1y)
Recommended
