
Results Table 1: Patient characteristics PowerPoint PPT Presentation
1 / 1
Title: Results Table 1: Patient characteristics
1
EFFECT OF AN ACUTE BOUT OF EXERCISE ON
INFLAMMATION IN CHILDREN WITH CYSTIC FIBROSIS
- Van de Weert van Leeuwen P.B.1, Beekman J.M.2,
Van der Ent C.K.1, Hulzebos H.J.1, Arets H.G.M.1 - Cystic Fibrosis Centre, University Medical Center
Utrecht, The Netherlands. - Molecular Immunology Lab, University Medical
Center Utrecht, The Netherlands.
Introduction Patients with cystic fibrosis (CF)
suffer from pulmonary infections predominantly
caused by Pseudomonas aeruginosa, leading to
tissue damage, a decline in lung function and
exercise capacity. Since exercise capacity has
been identified as an independent predictor of
morbidity and mortality in patients with CF,
cardiopulmonary exercise testing (CPET) has been
emphasized as important in evaluating and
assessing prognosis and disease management. In
healthy people exercise induces immunological
responses that mimic those induced by other
physical stressors. It induces transient
increases in leukocytes and cytokines. It has
been postulated that exercise induces immune
tolerance with a reduced capacity of phagocytes
to engulf bacteria, whereas others suggest the
opposite. Aim to investigate whether exercise
in patients with CF has an effect on 1
inflammatory markers, 2 serum dependent binding
and/ or phagocytosis of P. aeruginosa by
neutrophils.
Table 2 Differences in Leukocyte, leukocyte
subsets, CRP and IgG levels induced by
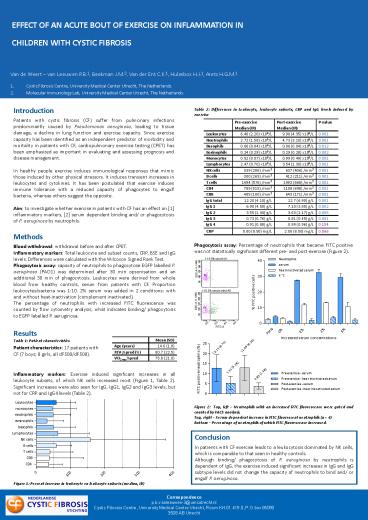
exercise Phagocytosis assay
Percentage of neutrophils that became FITC
positive was not statistically significant
different pre- and post-exercise (Figure
2). Figure 2 Top, left
Neutrophils with an increased FITC fluorescence
were gated and counted by FACS analysis.
Top, right Serum dependent increase in FITC
fluorescent neutrophils (n 4) Bottom
Percentage of neutrophils of which FITC
fluorescence increased.
Pre-exercise Median (IR) Post-exercise Median (IR) P-value
Leukocytes 6.40 (2.20) x109/L 9.90 (4.35) x109/L 0.001
Neutrophils 2.72 (1.58) x109/L 4.73 (3.10) x109/L 0.001
Basophils 0.06 (0.04) x109/L 0.06 (0.04) x109/L 0.012
Eosinophils 0.24 (0.29) x109/L 0.29 (0.28) x109/L 0.002
Monocytes 0.52 (0.07) x109/L 0.99 (0.49) x109/L 0.001
Lymphocytes 2.47 (0.70) x109/L 3.54 (1.30) x109/L 0.001
NK cells 339 (286) /mm3 637 (406) /mm3 0.001
B cells 300 (265) /mm3 412 (211) /mm3 0.001
T cells 1494 (576) /mm3 1992 (868) /mm3 0.001
CD4 789 (515) /mm3 1108 (698) /mm3 0.001
CD8 485 (180) /mm3 643 (171) /mm3 0.001
IgG total 12.20 (4.10) g/L 12.7 (6.90) g/L 0.001
IgG 1 6.90 (4.50) g/L 7.10 (3.85) g/L 0.002
IgG 2 3.55 (1.44) g/L 3.63 (2.17) g/L 0.005
IgG 3 0.73 (0.76) g/L 0.81 (0.45) g/L 0.001
IgG 4 0.91 (0.88) g/L 0.99 (0.96) g/L 0.154
CRP 0.00 (8.50) mg/L 2.00 (8.50) mg/L 0.066
Methods Blood withdrawal withdrawal before and
after CPET. Inflammatory markers Total
leukocyte and subset counts, CRP, BSE and IgG
levels. Differences were calculated with the
Wilcoxon Signed Rank Test. Phagocytosis assay
capacity of neutrophils to phagocytose EGFP
labelled P. aeruginosa (PAO1) was determined
after 30 min opsonisation and an additional 30
min of phagocytosis. Leukocytes were derived from
whole blood from healthy controls, serum from
patients with CF. Proportion leukocytesbacteria
was 110. 2 serum was added in 2 conditions
with and without heat-inactivation (complement
inactivated). The percentage of neutrophils with
increased FITC fluorescence was counted by flow
cytometry analysis, what indicates binding/
phagocytosis to EGFP labelled P. aeruginosa.
Results Table 1 Patient characteristics Pati
ent characteristics 17 patients with CF (7
boys 8 girls, all dF508/dF508). Inflammatory
markers Exercise induced significant increases
in all leukocyte subsets, of which NK cells
increased most (Figure 1, Table 2). Significant
increases were also seen for IgG, IgG1, IgG2 and
IgG3 levels, but not for CRP and IgG4 levels
(Table 2). Figure 1 Percent
increase in leukocyte en leukocyte subsets
(median, IR)
Mean (SD)
Age (years) 14.6 (1.8)
FEV1pred () 80.7 (22.5)
VO2maxpred 75.8 (21.0)
Conclusion In patients with CF exercise leads to
a leukocytosis dominated by NK cells, which is
comparable to that seen in healthy controls.
Although binding/ phagocytosis of P. aeruginosa
by neutrophils is dependent of IgG, the exercise
induced significant increases in IgG and IgG
subtype levels did not change the capacity of
neutrophils to bind and/ or engulf P. aeruginosa.
Correspondence p.b.vanleeuwen-3_at_umcutrecht.nl Cyst
ic Fibrosis Centre, University Medical Centre
Utrecht, Room KH.01.419.0, P.O.box 85090 3508 AB
Utrecht
Recommended
