
Results PowerPoint PPT Presentation
1 / 1
Title: Results
1
Compliance with Breast Cancer Screening
Guidelines in the HIV ClinicA Quality
Improvement ToolE. Patrozou M.D., E. Christaki
M.D., L. Hicks D.O., C. Wang M.D., F. Gillani
Ph.D., and K. Tashima M.D. Division of
Infectious Diseases, The Miriam Hospital, Alpert
Medical School of Brown University, Providence,
RI
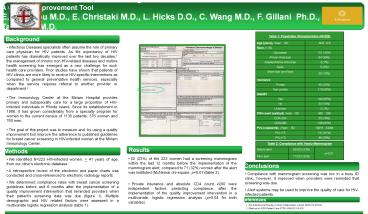
Table 1 Population Characteristics (N223) Table 1 Population Characteristics (N223)
Age (years), mean SD 49.6 6.6
Race, n ()
Caucasian 101 (45)
African-American 84 (38)
Alaskan/Native American 3 (1)
Asian 5 (2)
More than one Race 30 (13)
Insurance
Private 45 (20)
Non-private 178 (80)
HAART
Yes 190 (85)
No 33 (15)
Unknown 2 (1)
CD4 count (cells/µl), mean SD 480 298
CD4lt200 35 (16)
CD4200 188 (84)
PVL (copies/ml), mean SD 10018 34094
PVLlt75 137 (61)
PVL75 86 (39)
Background
- Infectious Diseases specialists often assume the
role of primary care physician for HIV patients.
As life expectancy of HIV patients has
dramatically improved over the last two decades,1
the management of chronic non HIV-related
diseases and routine health screening has emerged
as a new challenge for such health care
providers. Prior studies have shown that patients
of HIV clinics are more likely to receive
HIV-specific interventions as compared to general
preventative health services, especially when the
service requires referral to another provider or
department.2 - The Immunology Center at the Miriam Hospital
provides primary and subspecialty care for a
large proportion of HIV-infected individuals in
Rhode Island. Since its establishment in 1986, it
has grown considerably from a specialty program
for women to the current census of 1136 patients
376 women and 760 men. - The goal of this project was to measure and by
using a quality improvement tool improve the
adherence to published guidelines for breast
cancer screening in HIV-infected women at the
Miriam Immunology Center.
Methods
Table 2 Compliance with Yearly Mammogram Table 2 Compliance with Yearly Mammogram Table 2 Compliance with Yearly Mammogram
Before alert 52/223 (23) p0.01
After alert 71/223 (32) p0.01
Results
Methods
- 52 (23) of the 223 women had a screening
mammogram within the last 12 months before the
implementation of the mammogram alert, compared
to 71 (32) women after the alert was instituted
(McNemar chi-square, p0.01)(table 2). - Private insurance and absolute CD4 count 200
were independent factors predicting compliance
after the implementation of the quality
improvement intervention in a multivariate,
logistic regression analysis (p0.04 for both
variables).
- We identified N223 HIV-infected women, gt 41
years of age, from our clinics electronic
database. - A retrospective review of the electronic and
paper charts was conducted and cross-referenced
to electronic radiology reports. - We determined compliance rates with breast
cancer screening guidelines before and 6 months
after the implementation of a quality improvement
intervention that reminded providers when their
patients screening date was due (figure 1).
Multiple demographic and HIV related factors were
assessed in a multivariate logistic regression
analysis (table 1).
Conclusions
- Compliance with mammogram screening was low in a
busy ID clinic, however, it improved when
providers were reminded that screening was due. - Alert systems may be used to improve the quality
of care for HIV-infected patients.
References
1. The Antiretroviral Therapy Cohort
Collaboration, Lancet 2008372293-99 2 .Sheth et
al, AIDS Patient Care STDS 200620318-325
Recommended
