
The Excretory System PowerPoint PPT Presentation
1 / 46
Title: The Excretory System
1
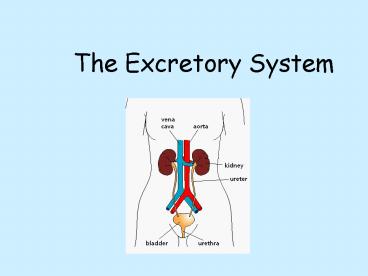
The Excretory System
2
- Excretion is the removal of the waste products of
metabolism from living organisms. - The accumulation of these waste products would be
toxic if they were not eliminated. - In plants and simple animals, waste products are
removed by diffusion. Plants, for example,
excrete O2, a product of photosynthesis.
3
METABOLIC WASTE A BY-PRODUCT OF
Water Dehydration synthesis and cellular respiration
Carbon dioxide Cellular respiration
Salts Neutralization reactions
Urea Deamination (removal of amino group from amino acids
Uric acid Nucleic acid breakdown
4
Organs of Excretion
- There are four major organs involved in
excretion - 1. The lungs
- 2. The liver
- 3. The skin
- 4. The kidneys
5
THE LUNGS
- Cellular respiration occurs in every living cell
in your body. - Carbon dioxide is produced as a waste product.
As the carbon dioxide accumulates in body cells,
it eventually diffuses out of the cells and into
the bloodstream, which eventually circulates to
the lungs. - In the alveoli of the lungs, carbon dioxide
diffuses from the blood, into the lung tissue,
and then leaves the body every time we exhale.
Some water vapor also exits the body during
exhalation.
6
THE SKIN
- As you already know, sweat comes out of pores in
your skin. - Sweat is a mixture of three metabolic wastes
water, salts, urea. - So as you sweat, your body accomplishes two
things - 1) sweating has a cooling effect on the body,
- 2) metabolic wastes are excreted.
7
- The skin is made up of two layers
- 1. The thin epidermis at the top
- 2. The thicker dermis below. This is where
oil glands, hair follicles, fatty layers, nerves,
and sweat glands are found.
8
- The sweat gland is a tubular structure tangled
with capillaries (the smallest of blood vessels). - This close association of tubes allows wastes
(water, salts urea) to diffuse from the blood
into the sweat gland. - When body temperature rises, the fluid (sweat) is
released from the gland, travels through the
duct, and reaches the skin surface through
openings called pores.
9
(No Transcript)
10
THE LIVER
- The liver is a large, important organ. In fact
it is the largest internal organ in our bodies.
Its numerous functions make it "part" of the
circulatory, digestive, and excretory systems. - In excretion, the liver removes the NH2 from
amino acids in proteins. This is called
deamination
11
- The by-product of deamination is ammonia, a
water-soluble gas. - Ammonia is extremely toxic so it is combined with
CO2 to make urea. - Urea is much less toxic and can dissolve in the
blood for excretion through the sweat or through
urine. - Uric acid is formed by the breakdown of nucleic
acids in the liver.
12
THE KIDNEY
- The kidney is the major organ of excretion.
- The kidney is also a major regulatory organ.
- Through the formation of urine, it is
responsible for the following - Removal of organic wastes urea, uric acid and
the breakdown products of hemoglobin and hormones - Regulation of concentrations of important ions
sodium, potassium, calcium, magnesium, sulfate
and phosphate ions
13
- Regulation of pH balance of body control levels
of H, HCO3- and NH4 - Regulation of Red Blood Cell production. The
kidneys release erythropoietin, which regulates
the production of RBCs in the bone marrow. - Regulation of blood pressure regulation of
fluid volume of the body. - Limited control of blood glucose and blood amino
acid concentration eliminate excess amounts
14
Structure of the Kidney
15
- Renal Capsule A smooth semitransparent membrane
that adheres tightly to the outer surface of the
kidney. - Renal Cortex The region of the kidney just below
the capsule. This part of the kidney is rich is
arterioles and venules.
16
- Renal Medulla The region below the cortex that
is segregated into triangular regions. The
triangular regions are the renal pyramids, which
are striated (or striped) in appearance due to
the collecting ducts running through them. - Renal Pelvis A cavity within the kidney that is
continuous with the ureter. The pelvis has
portions that extend towards the renal pyramids.
These extensions are called calyces.
17
(No Transcript)
18
The Nephron
- The functional unit of the kidney is the nephron.
Each kidney contains over one million of these
microscopic filters. - About 20 of the total blood pumped by the heart
each minute will enter the kidneys to undergo
filtration. This is called the filtration fraction
19
The nephron
20
Urine Formation
- Occurs in the nephron through three processes
- Glomerular Filtration
- Tubular Reabsorption
- Tubular Secretion
21
(No Transcript)
22
Glomerular filtration
- The transfer of fluid and solutes from the
glomerular capillaries into Bowmans capsule. - Blood enters the glomerulus under pressure. This
causes water, small molecules (urea, glucose,
amino acids) and ions to filter through the
capillary walls into Bowmans capsule. - Large blood components (RBCs, WBCs, platelets
and proteins) cannot filter through.
23
- The fluid in the Bowman's capsule appears very
much like interstitial fluid without the
proteins. It is called the nephric filtrate - The glomerular capillaries are substantially more
(100 to 1000X) leaky than regular capillaries and
have 2-3 times more pressure than regular
capillaries. - Glomerular filtration rate is fairly constant.
(130 ml/min or 7.8 l/hr). This means that about
190 L of filtrate is formed every 24 hours by
both kidneys
24
Tubular Reabsorption
- Occurs in the Proximal convoluted tubule, the
Loop of Henle and the Distal convoluted Tubule. - Materials which are required by the organism are
returned to the bloodstream water, ions,
glucose, amino acids etc - The kidney does not work by a process of
identifying what is bad rather it works by
identifying those things that are good for the
body
25
- Much of the urea is lost simply because the
kidney chooses not to recover it after it has
been filtered. - Any small foreign molecule that has entered our
blood, even if it has not existed in human
evolutionary history (drugs, new pollutants, etc)
can be removed by the kidney.
26
Proximal convoluted tubule
- The cells of the tubule are lined with
microvilli. Why? - Reabsorption of glucose, amino acids, and most
inorganic salts occurs here.
27
- Na ions are transported out of the tubule by
active transport, through carrier molecules. - Cl- ions and HCO3- ions follow by charge
attraction. - As these solutes move out of the tubule, they
create an osmotic gradient and water moves out of
the tubule and back into the blood, through
osmosis. - About 80-85 of the water in the filtrate is
reabsorbed in the proximal tubule.
28
- Glucose and amino acids attach to carrier
molecules and are transported out by active
transport. - This requires a lot of energy so there are many
mitochondria in the cells of the proximal tubule. - There is a limit to the amount of sodium, glucose
and amino acids that can be reabsorbed by the
carrier molecules the threshold limit. When
this limit is reached, these substances are
excreted in the urine.
29
- H ions are secreted into the proximal tubule.
This helps regulate pH. - About 50 of the urea that was in the nephric
filtrate is reabsorbed in the tubule. This is a
passive mechanism. The rest is excreted in the
urine.
30
The loop of Henle
- The descending loop of Henle is permeable to
water. Water is reabsorbed into the peritubular
capillaries by osmosis. - The filtrate decreases in volume,but increases in
osmotic concentration. - Salt (NaCl) becomes concentrated in the filtrate
as the loop penetrates the inner medulla of the
kidney.
31
- The ascending loop of Henle is permeable to salt
but not to water. Sodium is actively transported
out of the filtrate and chlorine follows by
charge attraction. - The volume of the filtrate does not change, but
the concentration decreases. - The peritubular capillaries ensure a rich blood
supply for reabsorption
32
The Distal Convoluted Tubule
- More sodium is reclaimed by active transport, and
still more water follows by osmosis. - Although 97 of the sodium has already been
removed, it is the last 3 that determines the
final balance of sodium. - This determines the water content and blood
pressure in the body. - The reabsorption of sodium in the distal tubule
and the collecting tubules is closely regulated,
chiefly by the action of the hormone aldosterone.
33
The Collecting Duct.
- The filtrate now flows into the collecting duct,
which gathers fluid from many nephrons. - Urine flows from the collecting ducts into the
renal pelvis to the ureters and into the bladder.
34
- Water regulation occurs here.
- The plasma membranes of the cells of the distal
tubule and the collecting duct have transmembrane
channels made of a protein called aquaporin. - When these channels are open, water can pass
through very quickly. These water channels are
responsive to levels of antidiuretic hormone
(ADH).
35
Tubular secretion
- This is the third mechanism of excretion.
- Secretion occurs when substances are transported
from the blood directly into the distal tubule. - Hydrogen, potassium, and ammonium ions are
actively secreted into the tubule. This helps to
regulate pH.
36
- If the pH of the blood becomes too acid, more H
ions are secreted into the tubule. - If the pH of the blood becomes too alkaline, then
secretion of H is reduced. - The pH of urine can vary from 4.5 to 8.5
- Certain drugs, such as penicillin, are also
secreted into the tubule for excretion. - Secretion occurs in the proximal tubule, the
distal tubule and the collecting duct.
37
- While we think of the kidney as an organ of
excretion, it is more than that. - It does remove wastes, but it also removes normal
components of the blood that are present in
greater-than-normal concentrations and reclaim
these components when they are present in the
blood in less-than-normal amounts. - Thus the kidney continuously regulates the
chemical composition of the blood within narrow
limits. The kidney is one of the major
homeostatic devices of the body.
38
Urine Testing
- Color Normal urine will vary from light straw to
amber color. - The color of normal urine is due to a pigment
called urochrome, which is the end product of
hemoglobin breakdown - Hemoglobin ? hematin ? bilirubin
?urochromogen ? urochrome
39
- The following changes in colour have pathological
implications - a. Milky presence of pus, bacteria, fat.
- b. Reddish amber presence of urobilinogen or
porphyrin. Urobilinogen is produced in the
intestine by the action of bacteria on bile
pigments. Porphyrin may be evidence of liver
cirrhosis, jaundice, Addison's disease, and other
conditions. - c. Brownish yellow or green presence of bile
pigments. - d. Red to smoky brown presence of blood and
blood pigments.
40
- Carrots may cause increased yellow color due to
carotene, while beets cause reddening and rhubarb
may cause the urine to become brown. These food
items and certain drugs may color the urine, yet
have no pathological significance.
41
Glucose
- glucose is not normally present in the urine
because all of it is usually reabsorbed from the
renal tubules into the blood. - When the glucose concentration of the filtrate is
within the normal limits (70-110 mg per 100 ml),
there is a sufficient number of carrier molecules
in the renal tubules to transport all the glucose
back into the blood.
42
- However, if the blood glucose level exceeds its
threshold (for glucose, about 180 mg per 100 ml),
there will not be enough carrier molecules to
reabsorb all of the glucose. - The untransported glucose will end up in the
urine and result in a condition known as
glycosuria. - The main cause of glycosuria is diabetes mellitus
43
Ketones (Ketonuria)
- Normally, no ketones are present in urine.
- Detectable levels of ketone may occur in urine
during physiological stress conditions such as
fasting, pregnancy, and frequent strenuous
exercise. - When there is carbohydrate deprivation, such as
in starvation or high-protein diets, the body
relies increasingly on the metabolism of fats for
energy.
44
- This pattern is also seen in people with diabetes
mellitus, where the lack of insulin prevents the
body cells from utilizing the large amounts of
glucose available in the blood. - When the production of the intermediate products
of fatty acid metabolism (ketone bodies) exceeds
the ability of the body to metabolize these
compounds, they accumulate in the blood and spill
over into the urine (ketonuria).
45
pH
- Freshly voided urine is usually acidic (around pH
6) but the normal range is between 4.8 and 7.5. - The pH will vary with the time of day and diet.
High acidity is present in acidosis, fevers, and
high protein diets. Excess alkalinity may be due
to urine retention in the bladder, chronic
cystitis, anemia, and obstructing gastric ulcers.
46
Protein
- Since proteins are very large molecules, they are
not normally present in measurable amounts in the
glomerular filtrate or the urine. - The detection of proteins in the urine,
therefore, may indicate that the permeability of
the glomerulus is abnormally increased. - This may be caused by renal infections
(nephritis), or it may be caused by other
diseases that affect the kidney,such as diabetes
mellitus, jaundice, or hyperthyroidism.
Recommended
