
Supplementary Table 1. - PowerPoint PPT Presentation
1 / 15
Title:
Supplementary Table 1.
Description:
Supplementary Table 1. Selected reference drugs, testing concentrations and therapeutic exposure a Ceff, the maximal therapeutic plasma concentration reported in the ... – PowerPoint PPT presentation
Number of Views:72
Avg rating:3.0/5.0
Title: Supplementary Table 1.
1
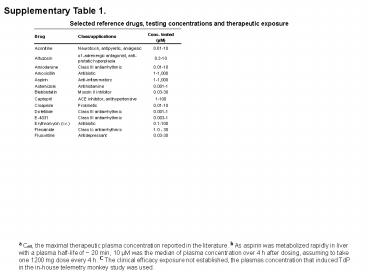
Supplementary Table 1.
Selected reference drugs, testing concentrations
and therapeutic exposure
a Ceff, the maximal therapeutic plasma
concentration reported in the literature. b As
aspirin was metabolized rapidly in liver with a
plasma half-life of 20 min, 10 µM was the
median of plasma concentration over 4 h after
dosing, assuming to take one 1200 mg dose every 4
h. C The clinical efficacy exposure not
established, the plasmas concentration that
induced TdP in the in-house telemetry monkey
study was used.
2
Supplementary Figure 1.
Suppl Fig. 1 Illustration of Irregular Beat
Ratio (IBR) calculation. The screen-shots were
taken from a 20 s-sweep window after exposure to
the vehicle (0.1 DMSO, top trace) and E-4031 at
30 nM (middle trace) and 1000 nM (bottom trace),
respectively. The regular (R) and irregular (I)
beats were denoted by the blue-dots and
red-arrowheads, respectively. The total (T) beats
was a sum of R and I in each sweeps, and the IBR
was calculated as the ratio of I/T.
3
Supplementary Figure 2.
Amoxicillin
A
Pre-drug Post-drug 30 min
1 h 6 h
24 h
72 h
0 µM 1 10 100
10 s
Captopril
B
Pre-drug Post-drug 30 min
1 h 6 h
24 h
72 h
0 µM 1 10 100
10 s
Suppl Fig. 2 Representative impedance traces for
amoxicillin and captopril. No obvious irregular
beats nor significant alteration in beat
amplitude were observed during drug exposure from
1 to 100 µM and up to 72 h. The vertical scale
bar 0.08 CI.
4
Supplementary Figure 3.
E-4031
A
Pre-drug Post-drug 30 min
1 h 6 h
24 h
72 h
0 nM 1 3 10 30 100 300 1000
B
Suppl Fig. 3 Dose- and time-dependent induction
of arrhythmic beats by E-4031. A) Representative
traces of RTCA Cardio recordings illustrate the
development of the single, double, triple and
short-train arrhythmic beats (denoted by
arrowheads) that are induced dose-dependently by
E-4031. Note, synchronous beats are arrested
completely at 24 h and 72 h by 1000 nM, and at 72
h by 300 nM. The vertical scale bar 0.1 CI.
B) The Irregular Beat Ratio averaged from 3
e-plates (3 wells/conc.) was plotted as a
function of time, demonstrating the rapid
induction of arrhythmic beats that are persistent
throughout the observation period at
concentrations 100 nM. The standard error bars
are not graphed for better clarity.
RTCA Cardio (n 3)
Conc. (nM)
5
Supplementary Figure 3.
E-4031
C
D
MEA (n 7)
Suppl Fig. 3 Dose- and time-dependent induction
of arrhythmic beats by E-4031. C) Representative
traces of microelectrode array (MEA) recordings
illustrate the development of the single, double,
triple and short-train arrhythmic beats (denoted
by arrowheads) induced dose-dependently by
E-4031. D) The Irregular Beat Ratio averaged
from 7 MEA wells was plotted as a function of
concentrations to demonstrate the dose-dependent
increase in arrhythmic beats induced by E-4031.
6
Supplementary Figure 4.
RO5657
A
Pre-drug Post-drug 30 min
1 h
6 h 24 h
72 h
0 µM 0.1 0.3 1 3 10 30 100
B
Suppl Fig. 4 Dose- and time-dependent induction
of arrhythmic beats by RO5657. A) Representative
traces of RTCA Cardio recordings illustrate the
development of typical arrhythmic beats (denoted
by arrowheads), ventricular fibrillation or
tachycardia-like (dark stars) arrhythmia that are
induced dose-dependently by RO5657. Note,
synchronous beats are arrested completely at 72 h
by 100 µM. The vertical scale bar 0.12 CI. B)
The Irregular Beat Ratio averaged from 5 e-plates
(5 wells /conc.) was plotted as a function of
time to demonstrate the quick induction and
dynamic change of arrhythmic beats throughout the
observation period up to 72 h. The standard error
bars are not graphed for better clarity.
RTCA Cardio (n 5)
Conc. (µM)
Irregular Beat Ratio
Beat-rate Irregular Ratio
7
Supplementary Figure 4.
RO5657
C
D
MEA (n 4)
Irregular Beat Ratio
Suppl Fig. 4 Dose- and time-dependent induction
of arrhythmic beats by RO5657. C) Representative
traces of microelectrode array (MEA) recordings
illustrate the development of typical arrhythmic
beats (denoted by arrowheads) induced
dose-dependently by RO5657. D) The plot of
Irregular Beat Ratio averaged from 4 MEA wells as
a function of concentrations demonstrates the
dose-dependent increase in arrhythmic beats
induced by RO5657.
8
Supplementary Figure 5.
Terfenadine
A
Pre-drug Post-drug 6 h
12 h 24 h
48 h
72 h
0 µM 0.01 0.03 0.1 0.3 1 3 10
Suppl Fig. 5 Dose- and time-dependent induction
of arrhythmic beats by terfenadine. A)
Representative traces of RTCA Cardio recordings
illustrate the quick arrest of synchronous
beatings and the development of typical
arrhythmic beats (denoted by arrowheads) and
ventricular fibrillation-like arrhythmia (dark
stars) induced dose-dependently by terfenadine.
Note, the time-dependent recovery of synchronous
beats at concentrations 1 µM and the delayed
induction of arrhythmic beats at concentrations
0.3 µM. The vertical scale bar 0.1 CI. B) The
Irregular Beat Ratio averaged from 3 e-plates (3
wells/conc.) was plotted as a function of time to
demonstrate the delayed induction of arrhythmic
beats. Arrhythmic beats occur after 12 h in
exposure to terfenadine. The standard error bars
are not graphed for better clarity.
B
Conc. (µM)
RTCA Cardio (n 3)
Irregular Beat Ratio
9
Supplementary Figure 6.
Thioridazine
A
Pre-drug Post-drug 6 h
12 h 24 h
48 h
72 h
0 µM 0.01 0.03 0.1 0.3 1 3 10
B
Suppl Fig. 6 Dose- and time-dependent induction
of arrhythmic beats by thioridazine. A)
Representative traces of RTCA Cardio recordings
illustrate the quick arrest of synchronous
beatings and the development of typical
arrhythmic beats (pointed with arrow heads)
dose-dependently by terfenadine. Note, the
time-dependent recovery of synchronous beats at
10 µM and the delayed induction of arrhythmic
beats at concentrations 3 µM. The vertical
scale bar 0.12 CI. B) The Irregular Beat
Ratio averaged from 3 e-plates (3 wells/conc.)
was plotted as a function of time to demonstrate
the delayed induction of arrhythmic beats.
Arrhythmic beats occur after 48 h in exposure to
thioridazine. The standard error bars are not
graphed for better clarity.
Conc. (µM)
RTCA Cardio (n 3)
Irregular Beat Ratio
10
Supplementary Figure 7.
Ranolazine
A
Pre-drug Post-drug 30 min
3 h 6 h
24 h
72 h
0 µM 0.01 0.03 1 3 10 30 100
B
Suppl Fig. 7 Dose- and time-dependent induction
of arrhythmic beats by ranolazine. A)
Representative traces of RTCA Cardio recordings
illustrate the slow development of typical
arrhythmic beats (denoted by arrowheads) induced
dose-dependently by ranolazine. Note, the
frequent occurrence of arrhythmic beats at 3 h
after exposure to the drug. The vertical scale
bar 0.08 CI. B) The plot of Irregular Beat
Ratio averaged from 5 e-plates (5 wells/conc.) as
a function of time demonstrates the slowly
developed and transient induction of arrhythmic
beats. Arrhythmic beats occur most frequently at
3 h after drug exposure.
Conc. (µM)
RTCA Cardio (n 5)
11
Supplementary Figure 8.
Verapamil
Pre-drug Post-drug 3 h
18 h 24 h
48 h
72 h
0 nM 10 30 100 300
10 s
Suppl Fig. 8 Dose- and time-dependent effects of
verapamil. Reduction in beat amplitude and
acceleration in beat rate were observed
immediately after drug addition. Both changes
recovered slowly and a complete recovery achieved
at 48 h post-drug exposure. The vertical scale
bar 0.08 CI.
12
Supplementary Reference
- Ogata, N., Narahashi, T. Block of sodium
channels by psychotropic drugs in single
guinea-pig cardiac myocytes. British J Pharmacol,
97, 905-913. (1989). - Wada, K., et al. Effects of long-term
administrations of aconitine on electrocardiogram
and tissue concentrations of aconitine and its
metabolites in mice. Forensic Sci International,
148, 21-29. (2005). - Lacerda, A.E. et al. Alfuzosin delays cardiac
repolarization by a novel mechanism. J Pharmacol
Exp Ther. 324(2), 427-33. (2008). - Redfern, W.S. et al. Relationships between
preclinical cardiac electrophysiology, clinical
QT interval prolongation and torsade de pointes
for a broad range of drugs evidence for a
provisional safety margin in drug development.
Cardiovascular Res, 58, 32-45. (2003). - Lawrence, C.L., et al. A rabbit Langendorff heart
proarrhythmia model predictive value for
clinical identification of Torsades de Pointes.
British J of Pharmacol, 149, 845-860. (2006). - Seymour, R.A., Rawlins, M.D. Efficacy and
pharmacokinetics of aspirin in post-operative
dental pain. Br J Clin Pharmacol. 13(6), 807-10.
(1982). - Selden, R., Neill, W. A. Myocardial uptake of
ouabain in intact dog and man. J Pharmacol Exp
Ther, 193, 951-962. (1975). - Fossa, A. A., et al. Differential effect of HERG
blocking agents on cardiac electrical alternans
in the guinea pig. Eur J Pharmacol. 486(2),
209-21. (2004). - FDA label (2006) for Ranexa
- http//129.128.185.122/drugbank2/drugs/DB0024
3/fda_labels/147 - 10. FDA label (1999) for Avelox
- http//129.128.185.122/drugbank2/drugs/DB0
0218/fda_labels/389 - 11. FDA label (1999) for Vioxx
- http//129.128.185.122/drugbank2/drugs/DB0
0533/fda_labels/980
13
Supplementary Video 1 (legend)
- Supplementary Video 1 Representative videos
depicting the contractility reduction of
Blebbistatin, a myosin II Inhibitor on human
iPSC-CMs. The 20 s video on the left shows
pre-drug, iPSC-CMs beating at their typical rate
and contraction. The 20 s video on the right
depicts the same field of cells as on the left,
after 15 min exposure of 1 µM Blebbistatin.
While robust contractions are evident on the
left, the contraction is severely reduced yet
still present in the video on the right, in
accordance with impedance traces. Additionally,
focusing on specific cells present in both the
left and right videos, it is apparent that there
is no change in the beat rate, in accordance with
both impedance and MEAs. For example, note the
large, dark round cell cluster in the lower right
corner of both videos this cluster is beating at
the same rate in both videos but the contraction
is significantly muted in the right post-drug
video. The cells depicted are plated onto an
ordinary 96-well tissue culture plate in order to
not have visuals imposed upon by impedance
electrodes at 10 X magnification.
14
Supplementary Video 2 (legend)
- Supplementary Video 2 Representative video
depicting the proarrhythmic effect of E-4031, a
specific hERG inhibitor on iPSC-CMs. The 17 s
video on the left shows pre-drug, iPSC-CMs
beating with a consistent rate, size of the
contraction and duration of each individual beat.
The 17 s video on the right depicts the same
field of cells as on the left, after 1 h exposure
of 0.03 µM E-4031. Both videos begin with the
onset of the first beat, with all beats numbered
in yellow text. In the pre-drug movie, the entire
field of cardiomyocytes beat synchronously at a
regular frequency, approximately once every two
seconds, for a total of 11 beats. In contrast,
after E-4031 treatment, the same field of cells
exhibit asynchronous beating, with a reduced
frequency of large contractions and many smaller
contracting, beats or twitches of single cells
for at least a combined 15 regular and irregular
beats/small twitches. These differences are best
observed by looping the movie playback and
observing each field separately. The cells
depicted are plated onto glass cover slips in
order to not have visuals imposed upon by
impedance electrodes at 10 X magnification.
15
Supplementary Video 3 (legend)
- Supplementary Video 3 Representative videos
depicting the fibrillation-like arrhythmia
induced by ouabain, a Na/K-ATPase inhibitor on
iPSC-CMs. The 20 s video on the left shows
pre-drug, iPSC-CMs beating at their typical rate
and contraction. The 20 s video on the right
depicts the same field of cells as on the left,
after 15 min exposure of 0.3 µM ouabain. A
synchronous monolayer of cells is visible on the
left video under pre-drug conditions. On the
right, ouabain caused very rapid and asynchronous
(fibrillation-like) contractions of individual
cells. The cells depicted are plated onto an
ordinary 96-well tissue culture plate in order to
not have visuals imposed upon by impedance
electrodes at 10 X magnification.
Recommended
CrystalGraphics Presentations





























