
Fungi by the Tristram scheme - PowerPoint PPT Presentation
1 / 45
Title:
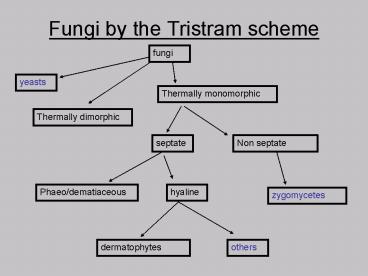
Fungi by the Tristram scheme
Description:
In the past, all fungi were categorised as pathogens or saprophytes: ... Mycology Review. Fungal structure. Yeasts vs moulds vs dimorphism. Birds and the bees ... – PowerPoint PPT presentation
Number of Views:115
Avg rating:3.0/5.0
Title: Fungi by the Tristram scheme
1
Fungi by the Tristram scheme
2
Opportunistic Fungal Infections (M8.1)with minor
updates sorry!
- In the past, all fungi were categorised as
pathogens or saprophytes those days are gone
forever. - Hyaline hyphomycetes
- Aspergillus, Scedosporium, Fusarium, others.
- Zygomycetes
- Mucor, Rhizopus, Rhizomucor, others.
3
Common factors (M8.2)
- Common in environment.
- Abundant conidia / release, and therefore
frequent airborne contaminants. - Grow rapidly.
- Initial entry is usually pulmonary (for systemic
disease). - Interpretation of culture can be a problem
- Contaminant, coloniser, infection?
4
Hyaline hyphomycetes (M8.3)
- Colourless septate hyphae and pigmented conidia
(if thallus is pigmented) - Important genera
- Aspergillus (green to black)
- Scedosporium (Pseudallescheria)
- also rans
- Fusarium (pinkish)
- Paecilomyces (pinkish)
- Penicillium (green to brown)
5
Penicillium spp. (M8.4)
- Nearly always a contaminant
- Important to recognise
- Has NO vesicle.
6
(No Transcript)
7
(No Transcript)
8
Aspergillosis (M8.5)
- 600 species, 20 in humans, 4 common
- A. fumigatus, flavus, niger, terreus
- Identification
- Macroscopic morphology (pigmentation)
- Microscopy
- Head coverage
- Length of conidiophore
- Uniseriate or biseriate
9
(No Transcript)
10
Aspergillosis (M8.6)
- Clinical manifestations
- Contaminant
- Superficial
- Otomycosis and keratitis
- Respiratory
- Colonising, allergic, aspergilloma, acute
invasive. - Disseminated
- Immunosuppressed, nosocomial
11
Laboratory diagnosis (M8.7)
- Direct microscopy
- Helpful in establishing veracity of isolate.
- Septate, dich branching hyphae (non spec)
- Culture
- Non fastidious, but cyclohexamide S
- Problems with dissemination
- Non culture
- Antibody, antigen, metabolites, PCR
Invasive aspergillosis has a crude mortality rate
of 95, due to nature of patient AND to problems
in rapid diagnosis.
12
Impact of Early Diagnosis (M8.7a)(from Perfect
ASA 2004)
- Aspergillus pneumonia
- 10 d mortality 9/22 (41)
- gt10d mortality 9/10 (90)t
- Systematic CT scan (2d) 20 mortality
- on indication CT scan (7d) 58 mortality?
- t von Eiff et al, Resp. 1995
- ? Caillot et al, J. Clin. Oncol. 1997
13
(No Transcript)
14
037
15
Zygomycetes (M8.8)
- Mucor, Rhizopus, Rhizomucor
- Sexual stage has zygospores, but the asexual
stage is typical with BROAD non septate hyphae
and sporangia
16
(No Transcript)
17
Zygomycosis (8.9)
- Also called Mucormycosis
- Acquired by inhalation, affects neutropenics,
diabetics, malignancy - Can disseminate to any organ.
- VASCULAR INVASION and infarction.
- Rhinocerebral mucormycosis
- A special case, uncontrolled diabetes
18
582
19
580
20
Case Study
- Liang et al JCM 2006, 44,3.
- 50 year old diabetic.
- R eye pain and proptosis
- Debridement and amp B.
21
(No Transcript)
22
(No Transcript)
23
Agar flotation method
- A method apparently useful in making some of
the weakly sporulating Zygomycetes produce
spores. - Also use 1 water agar (D. Ellis)
- Probably amounts to fungal abuse
24
Zygomycosis (8.10)
- Laboratory diagnosis
- Urgency
- Direct microscopy typical
- Culture
- Can be negative after maceration.
- Very rapid growth.
25
585
26
(No Transcript)
27
586
28
Case Study
- Salinas et al, Lab Medicine, 2004, 335
- 24 year old male, motorcycle accident
- Facial laceration, facial and neck fractures,
bleeding from nares, SAH and SDH. - Day 4 wound culture grew E. coli and .
29
- Within 5 days colony filled plate.
- No fruiting bodies.
- Fontana-masson stain on Bx
- (?dermatiaceous sic)
30
- Day 9 necrosis on neck 72 hrs debride x 3.
- 1 water agar induction of sporulation.
31
- Apophysomyces elegans
- 15 body debridement topical/oral Amp B
32
Scedosporium spp.
- S. apiospermum (Pseudallescheria boydii)
- S. prolificans
- Both common causes of mycetoma worldwide
- Increasing incidence, esp in Aus of pulmonary and
disseminated disease. - Colonising airways - CF patients, lung Tx
- Dissemination in neutropenics
33
Treatment of Scedosporium infections
- Very very difficult.
- Both species are resistant to most commonly used
antifungal drugs. - Successful therapy often involves experimental
combinations of drugs.
34
524
35
525
36
529
37
530
38
Case study
- Kowacs et al J Clin Path 2004, 57.
- 32 year old male, post near drowning in pig
sewerage reservoir. - 15 days post, fever, headache.
- CT scan abscesses or granuloma.
- CTX, MTZ, fluconazole and discharged.
39
- 2 weeks later, returned CSF 1300 / mm3
- Mannitol, dexa, vanc, rif, ctx, carbamazepine.
- 2 days later, siezures, CSF 3000 / mm3
- Neg microbiology but suspect Scedosporium
- Add amphotericin B and itraconazole.
- Worsened clinically
- Neg Cryptococcus, amoebae, bacteria
- Finally grew Scedosporium apiospermum
- Dexa, clonaz, phenytoin, cefipime, vanv, MTZ,
fluc, amp B, intra-thecal miconazole. - Died 3 days later (3 months post pres)
40
Nosocomial fungal infections (M8.11)
- Increasing, and at a disproportionate rate to
other nosocomial infections. - Risk factors
- Immunosuppression
- profound and prolonged neutropenia following
chemotherapy - post transplant (bone marrow, heart are high)
- Increased access via catheters and other.
41
Nosocomial fungal pathogens (M8.12)
- Candida albicans
- 7th most common nosocomial pathogen!
- Fungaemia and dissemination
- Other yeasts
- Candida spp, and non Candida
- Aspergillus spp.
- Other emerging pathogens.
42
Nosocomial fungal infections (M8.13)
- Epidemiology
- Endogenous vs Exogenous
- Hepa filters, no plants
- Body surveillance for Candida albicans
- Outbreaks
- Airborne (construction)
- Cross infection minor issue
- Contamination - TPN
43
Nosocomial Fungal Infections (M8.14)
- Very high mortality
- 30 of deaths following prolonged neutropenia are
diagnosed with fungal infection post mortem. - 2x mortality if nosocomial fungal
- 50 crude mortality for Candidaemia.
- Poor diagnostic tools
- Relatively poor drugs (getting better)
- Non routine sens testing
- Contribution of host factors.
44
Fungi and air quality (M8.15)
- sick building syndrome
- Respiratory problems, sneezing, congestion,
cough, eyes burning, SOB - CNS problems, headaches
- Proliferation of moulds (moisture) and dispersal
of conidia. - Water bed!, pot plants, windows in cold climates,
air conditioning systems.
45
Mycology Review
- Fungal structure
- Yeasts vs moulds vs dimorphism
- Birds and the bees
- Superficial mycoses
- Cutaneous mycoses
- Subcutaneous mycoses
- Endemic systemic dimorphic mycoses
- Pathogenic yeasts
- Hyalohyphomycetes
- Zygomycetes
Recommended
CrystalGraphics Presentations





























