
Percutaneous tenontotomy of the Achilles tendon PowerPoint PPT Presentation
1 / 10
Title: Percutaneous tenontotomy of the Achilles tendon
1
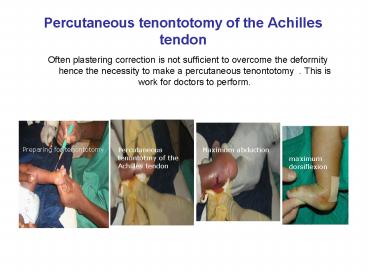
Percutaneous tenontotomy of the Achilles tendon
- Often plastering correction is not sufficient to
overcome the deformity hence the necessity to
make a percutaneous tenontotomy . This is work
for doctors to perform.
Preparing for tenontotomy
Percutaneous tenontotmy of the Achilles tendon
Maximum abduction
maximum dorsiflexion
2
Post plastering correction follow up
- Night splint wearing (Steenbeek) for the
maintenance of the correction - Daylight splint wearing (levator) for the
maintenance of the correction - Re-education (softening of the muscles if
necessary)
Attelle de nuit
Attelle de jour
Attelle de nuit
3
Results1 Health agents training
4
Results 2 Nomber of treated patients from
Octobre 2006 to February 2009 per centre
- Conclusion this chart shows that the male sex
is more often victim of the congenital deformity
than the female sex (PBVE).
5
Results 3 situation of the patients treated from
Octobre 2006 to February 2009
6
Results 4 Evaluation of performances Cases of
203 patients treated consisting of 80 bilateral
and 123 unilateral (68 right legs and 55 left
legs)
7
Results 4 Evaluation of performances
(continued)
- An analysis of these results shows that out of
1255 responses, we have - 1174 times where satisfaction has been reached at
least with the average of 3/5 that is 93,5
versus - 81 times with non satisfaction, that is 6,5
- As a conclusion, we can say that the Malian
experience as regards club foot with the Ponséti
method has been a 93,5 of C success
8
Obstacles met
- Despite these results we often meet with
difficulties that are generally related to - Accessibility of the treatment centres due to
distance - Treatement of equin varus club foot in the
centres where services are paid - Lack of parental home monitoring for plastered
children who often come back to us with defective
plasterings during the first phase of treatment - Regular wearing of night splints after the first
phase of treatment (plastering) - Lack of mastery in the making of night splints by
cobblers
9
Obstacles met (continued)
- Non respect of appointments for children follow
up after the first phase of treatment. - Availability of regular raw materials stocks
- Lack of mastery over the Ponséti method by
certain therapists . - Failur in some tenontotomy or operated cases
- Different methods of trainers in relation to day
light splint wearing - Frequency of recurrence
10
Thanks for helping me
Recommended
