
Dental Tissues and their Replacements - PowerPoint PPT Presentation
1 / 43
Title:
Dental Tissues and their Replacements
Description:
While many dental fixtures are not 'inside' the body, the environment (loading, ... Adhesive is dental cement. Permanent Abutment ... – PowerPoint PPT presentation
Number of Views:307
Avg rating:3.0/5.0
Title: Dental Tissues and their Replacements
1
Dental Tissues and their Replacements
2
Issues
- Dental decay
- Periodontal disease
- Movement of teeth (orthodontics)
- Restorative treatments
- Thermal expansion issues related to fillings
- Fatigue and fracture of teeth and implants
3
(No Transcript)
4
Marshall et al., J. Dentistry, 25,441, 1997.
5
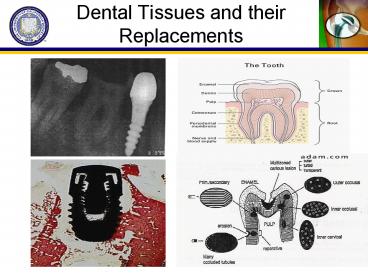
Tissue Constituents
- Enamel-hardest substance in body-calcium
phosphate salts-large apatite crystals - Dentin-composed largely of type-I collagen
fibrils and nanocrystalline apatite
mineral-similar to bone - Dentinal tubules-radiate from pulp
- Pulp-richly vascularized connnective tissue
- Cementum-coarsely fibrillated bonelike substance
devoid of canaliculi - Periodontal Membrane-anchors the root into
alveolar bone
6
ENAMEL
- 96mineral, 1 protein lipid, remainder is water
(weight ) - Minerals form Long crystals-hexagonal shape
- Flourine- renders enamel much less soluble and
increases hardness - HA Ca10(PO4)6(OH)2
40 nm 1000 nm in length
7
DENTIN
- Type-I collagen fibrils and nanocrystalline
apatite - Dentinal tubules from dentin-enamel and
cementum-enamel junctions to pulp - Channels are paths for odontoblasts
(dentin-forming cells) during the process of
dentin formation - Mineralized collagen fibrils (50-100 nm in
diameter) are arranged orthogonal to the tubules - Inter-tubular dentin matrix with nanocrystalline
hydroxyapatite mineral- planar structure - Highly oriented microstructure causes anisotropy
- Hollow tubules responsible for high toughness
8
Structural properties
Park and Lakes, Biomaterials, 1992 and Handbook
of Biomaterials, 1998
9
Structural properties
Note remodeling is primarily strain driven
Park and Lakes, Biomaterials, 1992 and Handbook
of Biomaterials, 1998
10
Dental Biomaterials
- Amalgams/Fillings
- Implants /Dental screws
- Adhesives/Cements
- Orthodontics
11
Materials used in dental applications
- Fillings amalgams, acrylic resins
- Titanium Ti6Al4V dominates in root implants and
fracture fixation - Teeth Porcelain, resins, ceramics
- Braces Stainless steel, Nitinol
- Cements/resins acrylate based polymers
- Bridges Resin, composite, metal (Au, CoCr)
12
Motivation to replace teeth
- Prevent loss in root support and chewing
efficiency - Prevent bone resorption
- Maintain healthy teeth
- Cosmetic
13
Amalgams/Fillings
- An amalgam is an alloy in which one component is
mercury (Hg) - Hg is liquid at RT- reacts with silver and tin-
forms plastic mass that sets with time - Takes 24 hours for full set (30 min for initial
set).
14
Thermal expansion concerns
- Thermal expansion coefficient
- ? ?L/(Lo?T)
- ? ? ?T
- Volumetric Thermal expansion coefficient
- V 3?
15
Volume Changes and Forces in Fillings
- Consider a 2mm diameter hole which is 4mm in
length in a molar tooth, with thermal variation
of ?T 50C - ?amalgam 25x10-6/C ?resin 81x10-6 /C
?enamel 8.3 x10-6 /C - E amalgam 20 GPa E resin 2.5 GPa
- ?V Vo x 3? x ?T
- ?Vamalgam p (1mm) 2 x 4mm x 3 (25-8.3) x10-6 x
50 - 0.03 mm3
- ?Vresin 0.14 mm3
- (1-d) F E x ?? x Afilling
- F E (?T ) ?(?amalgam/resin -
?enamel ) x p/4D2 - F amalgam 52 N S F/Ashear2.1 MPa
- F resin 29 N S 1.15 MPa
- Although the resin expands 4x greater than the
amalgam, the reduced stiffness (modulus) results
in a lower force
16
Volume Changes and Forces in Fillings(cont.)
- F amalgam 52 N S F/Ashear2.1 MPa
- F resin 29 N S 1.15 MPa
- Recall that tensile strength of enamel and dentin
are - sf,dentin35 MPa (worst case)
- sf,enamel7 MPa (distribution)
- From Mohrs circle, max. principal stress S
- -SF3.5! (What is SF for 3mm diameter?)
- - Is the change to resin based fillings
advisable? What are the trade-offs? - - We havent considered the hoop effect, is it
likely to make this worse? - - If KIc1 MPam1/2 , is fracture likely?
17
Environment for implants
- Chewing force can be up to 900 N
- Cyclic loading Large temperature differences (50
C) - Large pH differences (saliva, foods)
- Large variety of chemical compositions from food
- Crevices (natural and artificial) likely sites
for stress corrosion
18
Structural Requirements
- Fatigue resistance
- Fracture resistance
- Wear resistance
- Corrosion resistance
- While many dental fixtures are not inside the
body, the environment (loading, pH) is quite
severe
19
Titanium implants
- Titanium is the most successful implant/fixation
material - Good bone in-growth
- Stability
- Biocompatibility
20
Titanium Implants
- Implanted into jawbone
- Ti6Al4V is dominant implant
- Surface treatments/ion implantation improve
fretting resistance
- Osseointegration was coined by Brånemark, a
periodontic professor/surgeon - First Ti integrating implants were dental
(1962-1965)
21
Titanium Biocompatibility
- Bioinert
- Low corrosion
- Osseointegration
- Roughness, HA
22
Fatigue
- Fatigue is a concern for human teeth (1 million
cycles annually, typical stresses of 5-20 MPa) - The critical crack sizes for typical masticatory
stresses (20 MPa) of the order of 1.9 meters. - For the Total Life Approach, stresses (even after
accounting for stress concentrations) well
below the fatigue limit (600 MPa) - For the Defect Tolerant Approach, the Paris
equation of da/dN (m/cycle) 1x10-11(DK)3.9 used
for lifetime prediction. - Crack sizes at threshold are 1.5 mm (detectable).
23
Fatigue Properties of Ti6Al4V
24
(No Transcript)
25
Structural failures
- Stress (Corrosion) Cracking
- Fretting (and corrosion)
- Low wear resistance on surface
- Loosening
- Third Body Wear
26
(No Transcript)
27
Design Issues
- Internal taper for easy fitting
- Careful design to avoid stress concentrations
- Smooth external finish on the healing cap and
abutment - Healing cap to assist in easy removal
28
Surgical Process for Implantation
- Drill a hole with reamer appropriate to
dimensions of the selected implant at location
of extraction site
29
Temporary Abutment
- Place temporary abutment into implant
30
Insertion
- Insert implant
- with temporary abutment attached into prepared
socket
31
Healing
- View of temporary abutment after the healing
period (about 10 weeks)
32
Temporary Abutment Removal
- Temporary abutment removal after healing period
- Implant is fully osseointegrated
33
Healed tissue
- View of soft tissue before insertion of permanent
abutment
34
Permanent Crown Attached
- Abutment with all-ceramic crown integrated
- Adhesive is dental cement
35
Permanent Abutment
- Insert permanent abutment with integrated crown
into the well of the implant
36
Completed implant
- View of completed implantation procedure
- Compare aesthetic results of all-ceramic
submerged implant with adjacent protruding metal
lining of non-submerged implant
37
Post-op
- Post-operative radiograph with integrated
abutment crown in vivo
38
Clinical (service) Issues
- The space for the implant is small, dependent on
patient anatomy/ pathology - Fixation dependent on
- Surface
- Stress (atrophy)
- Bone/implant geometry
- Simulation shows partial fixation due to design
- (Atrophy below 1.5 MPa)
Vallaincourt et al., Appl. Biomat. 6 (267-282)
1995
39
Clinical Issues
- Stress is a function of diameter, or remaining
bone in ridge - Values for perfect bond
- Areas small
- Fretting
- Bending
40
Clinical Issues
- Full dentures may use several implants
- Bending of bridge, implants
- Large moments
- Fatigue!
- Complex combined stress
- FEA!
FBD
41
Clinical Issues
- Outstanding issues
- Threads or not?
- More surface area, not universal
- Immediately loaded
- Drilling temperature necrosis
- Graded stiffness
- Material or geometry
- Outcomes 80-95 success at 10-15 yrs.
- Many patient-specific and design-specific problems
42
Comparison with THR
- Compare
- Contrast
43
Comparison with THR
- Compare
- Stress shielding
- Graded stiffness/ integration
- Small bone section about implant
- Modular Ti design
- Morbidity
- Contrast
- Small surface area
- Acidic environment
- Exposure to bacteria
- Multiple implants
- Variable anatomy
- Complicated forces
- Cortical/ trabecular
- Optional
Recommended
CrystalGraphics Presentations





























