
Hierarchy of Clinical Evidence - PowerPoint PPT Presentation
Title:
Hierarchy of Clinical Evidence
Description:
Questions to ask when an association is reported in the literature (eg estrogen ... ACP J Club, Bandolier, POEMS, clinical evidence, Cochrane Reviews, Clinical ... – PowerPoint PPT presentation
Number of Views:150
Avg rating:3.0/5.0
Title: Hierarchy of Clinical Evidence
1
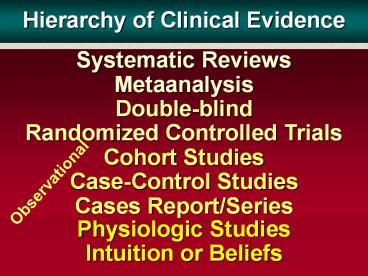
Hierarchy of Clinical Evidence
Systematic Reviews Metaanalysis Double-blindRando
mized Controlled Trials Cohort StudiesCase-Contro
l StudiesCases Report/Series
Physiologic Studies Intuition or Beliefs
Observational
2
Design of a cohort study
- TIME
- direction of inquiry
- people
exposed disease - population without the
no disease - disease
-
not exposed
disease -
no disease
at risk
3
Design of a case-control study
- TIME
- direction of inquiry
- Start with
- Exposed
cases (people -
with disease) - Not exposed
- Population
- Exposed
controls (people -
without disease) - Not exposed
4
Questions to ask when an association is reported
in the literature (eg estrogen and CHD)
- Explanation Finding
- Association
- Bias in selection Yes No
- or measurement
- Chance Likely Unlikely
- Confounding Yes No
- Cause Cause
5
Association and cause
Case report?
- Explanation Finding
- Association
- Bias in selection Yes No
- or measurement
- Chance Likely Unlikely
- Confounding Yes No
- Cause Cause
Case series?
6
Association and cause
- Explanation Finding
- Association
- Bias in selection Yes No
- or measurement
- Chance Likely Unlikely
- Confounding Yes No
- Cause Cause
P value
7
Association and cause
- Explanation Finding
- Association
- Bias in selection Yes No
- or measurement
- Chance Likely Unlikely
- Confounding Yes No
- Cause Cause
8
Criteria for causation
- 1. Is there evidence from true experimentation
in humans? - 2. Is the association strong?
- 3. Is the association consistent from study to
study? - 4. Is the temporal association correct?
- 5. Is there a dose-response gradient?
- 6. Does the association make biological sense?
- 7. Is the association specific?
- (Adapted from Bradford Hill)
9
Randomization
- 1. Guarantees equal probability of receiving
control/experimental treatment to all
participants (removes investigator bias) - 2. Protects against imbalances in known and
unknown confounders - 3. Provides basis for statistical analysis
10
Hierarchy of study methods for clinical
decision-making
Systematic reviews
11
Is observational evidence equivalent to
experimental evidence?
- Benson NEJM 20003421877
- Concato NEJM 20003421887
In some cases -YES
In others- NO !
12
Clinical trials are selective! -Select group gets
in - chance decides who gets treatment treatment
effect decides who does better
Observational evidence is also selective
self-selection of exposure this may decide who
does better
13
How much of Medicine is Evidence-Based ?
- Matzen P. Ugeskr laeger 20031651431-5
- General Internal Medicine - 50
- Psychiatry- 65
- Others (surgery, general practice, dermatology) -
less - Lai Br. J Ophthal . 20034385-90
- 42.9 of patient interventions were based on
evidence from RCT, meta-analysis or systematic
reviews (23 on no evidence)
14
Major Disadvantage of RCTsSelectivity
15
Clinical trials
- Should not be performed unless there is a
realistic chance of providing a valid/reliable
answer to a well-defined medical question
16
ButSHEP study
Of 447,921 (100) identified
31,960 (11.6) met initial criteria
4,736 (1.03) randomized
17
of Pop
Men, genl pop
DM CVD CHF MI Angina
Wom., genl pop
SHEP pop
18
Coke tastes better.!
Than what?
19
Coke tastes better.!
20
CAVEATS in using RCT evidence to guide patient
management
- 1. Tendency to extend application of new
treatments to patient groups other that those for
whom data exist
- 2. Extrapolation of data to agents of the same
class but untested for specific indication
21
Dont drown in the evidence
ACP J Club, Bandolier, POEMS,
clinical evidence, Cochrane Reviews,
Clinical guidelines
clearinghouse
Use predigested sources
22
Good luck!
Recommended
CrystalGraphics Presentations





























