
References PowerPoint PPT Presentation
1 / 2
Title: References
1
In-vitro Activity of the Novel
Ceragenin CSA 13 vs Multi-drug Resistant Strains
of Acinetobacter baumanniiWareham DW 1,2,
Genberg C 3 , Savage PB 4, Bean DC 11 2Centre
for Infectious Disease, Institute of Cell and
Molecular Science, Barts and The London, Queen
Marys School of Medicine and Dentistry, London,
UK 2Department of Medical Microbiology, Barts
and The London NHS Trust, London, UK 3
Ceragenix, Denver, CO, USA 4Brigham Young
University, Provo, UT
F1-1657
d.w.wareham_at_qmul.ac.uk
Abstract
Methods
MIC and MBCs to CSA-13 were determined by broth
microtitre dilution. The MIC50 of CSA-13 was 8
mg/L and the MIC90 16 mg/L. The MBC50 and MBC90
were 8 and 32 mg/L respectively (Figure 3). High
MIC and MBC (gt 128 mg/L) was exhibited by only 2
isolates.
Background Acinetobacter baumannii has emerged
as an important nosocomial pathogen causing burn
wound infections, ventilator associated
pneumonia, bacteremia and sepsis in the
critically ill. The organism exhibits formidable
multi-drug resistance with the isolates prevalent
in the UK characteristically resistant to all
ß-lactams (including carbapenems), ß-lactam /
inhibitor combinations, quinolones, and
aminoglycosides. In view of the lack of agents in
development for the treatment of MDR
Acinetobacters we set out to determine the
in-vitro activity of the novel cationic peptide
CSA-13 versus prevalent UK isolates. Methods
Seventy-two strains were identified as A.
baumannii by API 20NE and where necessary by
sequence analysis of the 16S rDNA gene.
Susceptibility to ampicillin, cefuroxime,
ceftriaxone, ciprofloxacin, trimethoprim,
piperacillin / tazobactam, gentamicin, amikacin,
aztreonam, ceftazidime, imipenem and colistin was
carried out using the BSAC disc diffusion method.
Genes encoding OXA carbapenemases (OXA-51, 23, 24
and 58) were amplified using multiplex PCR.
Inhibitory and bactericidal concentrations of
CSA-13 were determined by broth microtitre
dilution according to standard BSAC methodology.
Results All strains exhibited multi-drug
resistance to all antimicrobial classes tested
all with the exception of colistin and all except
one contained the OXA-51 and OXA-23 carbapenemase
genes. The MIC50 of CSA-13 was 8 mg/L and the
MIC90 16 mg/L. The MBC50 and MBC90 were 8 and 32
mg/L respectively. Conclusions The paucity of
agents active against A. baumannii requires
immediate development of alternatives. CSA-13
exhibits some activity versus the prevalent
strains of MDR A. baumannii in the UK, and CSA
compounds should be further investigated for this
purpose. Alternatively incorporation of CSA-13 at
supra-MIC concentrations into wound dressings or
medical devices or use as a topical or inhalation
therapy may be effective in achieving therapeutic
concentrations
72 isolates from various sites including
respiratory (n 47), wounds (n17), catheter tips
(n6) and blood (n2) were identified
biochemically as Acinetobacter baumannii.
Antimicrobial susceptibility testing was carried
out using the BSAC disc diffusion method and the
following agents ampicillin , amoxicillin /
clavulanate, cefpodoxime, cefuroxime, gentamicin,
ciprofloxacin, piperacillin / tazobactam,
amikacin, trimethoprim, aztreonam, ceftazidime,
imipenem, tobramycin, meropenem, sulbactam,
minocycline and colistin. Susceptibility was
determined by comparison of the zone sizes with
BSAC break points. Minimum Inhibitory
concentration (MIC) and minimum bactericidal
concentration (MBC) of CSA-13 were determined by
broth microtitre dilution. Multiplex PCR was used
to detect genes encoding for OXA-51, 23, 24 and
58 carbapenemase genes
Results
4mg/L
32 mg/L
8mg/L
16mg/L
gt128 mg/L
All isolates exhibited multidrug resistance
including resitance to carbapenems. The
susceptibility of the isolates to all 17 agents
and MIC and MBCs to CSA-13 is summarised in
Figure 1.
Figure 1 Susceptibility of A. baumannii to
antimicrobial agents
- CSA-13 exhibited promising activity versus
multidrug resistant strains of Acinetobacter
baumannii - The antimicrobial activity of the agent could be
exploited by incorporation into medical devices
such as urinary catheters or intravascular
devices or delivered to sites of infection by in
aerosolisation - Further structural modifications of CSA-13 may
lead to enhanced activity. - The agent is a promising candidate for further
therapeutic development.
Introduction
Acinetobacter baumannii is a non-fermentative
Gram negative rod belonging to the family
Moraxellaciae. In recent years it has emerged as
an important cause of nosocomial infection
responsible for pneumonia, wound infections,
bacteremia and sepsis in the immunosuppressed and
critically ill (Joly-Guillou, 2005). Many
clinical isolates exhibit marked antimicrobial
resistance severely limiting treatment options
(Poirel and Nordmann, 2006 Vila et al., 2007).
In London and the South East of England strains
resistant to all commonly used antibiotics i.e.
ß-lactams (including carbapenems),
fluoroquinolones, and aminoglycosides but
remaining consistently susceptible to the
antimicrobial peptide polymyxin B, have been
recovered with increasing frequency since 2001
(Coelho et al, 2004). The novel ceregenin CSA-13
is an antimicrobial peptide mimic with a steroid
backbone which has been shown to be active
in-vitro against a number of Gram-positive and
Gram-negative bacterial species (Figure 1). In
view of the dearth of agents active against
Multi-drug resistant Acinetobacter we set out to
determine the activity of CSA-13 versus prevalent
multi-drug resistant strains in the UK.
References
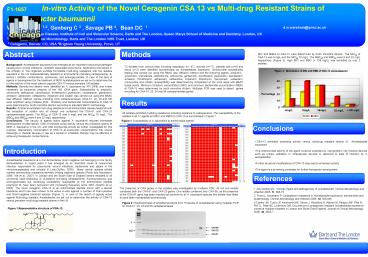
The presence of OXA genes in the isolates was
investigated by multiplex PCR. All but one
isolate contained both the OXA-51 and OXA-23
genes. One isolate contained only OXA-58, as the
presence of the OXA-51 gene has been reported as
common to all A. baumannii species this isolate
was lilkley to have been misidentified
biochemically
1. Joly-Guillou M-L. Clinical impact and
pathogenicity of Acinetobacter. Clinical
Microbiology and Infection 2005 11, 868-73 2.
Poirel L, Nordmann P. Carbapenem resistance in
Acinetobacter baumannii mechanisms and
epidemiology. Clinical Microbiology and Infection
2006 12, 826-836 3.Coelho JM, Turton JF,
Kaufmann ME, Glover J, Woodford N, Warner M,
Palepou MF, Pike R, Pitt TL, Patel BC, Livermore
DM. Occurrence of carbapenem resistant
Acinetobacter baumannii clones at multiple
hospitals in London and South East England.
Journal of Clinical Microbiology 2006, 44,
3623-7 .
Figure 2 Electrophoresis of amplified products
from 15 strains of Acinetobacter using multiplex
PCR for OXA-51, 23, 24 and 58 carbapenemases
Figure 1Representative structure of CSA-13
2
(No Transcript)
Recommended
