
Cardiac Imaging: Echo - PowerPoint PPT Presentation
1 / 31
Title:
Cardiac Imaging: Echo
Description:
Cardiac Imaging: Echo Blood moving away From transducer: Blue Blood moving toward Transducer: Red / Orange Turbulent blood flow: Green Echocardiogram uses – PowerPoint PPT presentation
Number of Views:636
Avg rating:3.0/5.0
Title: Cardiac Imaging: Echo
1
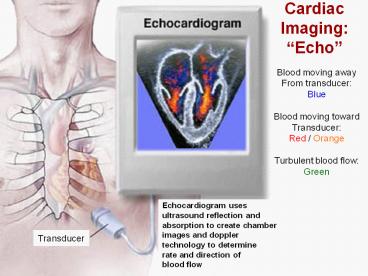
Cardiac ImagingEcho
Blood moving away From transducer Blue Blood
moving toward Transducer Red / Orange Turbulent
blood flow Green
Echocardiogram uses ultrasound reflection and
absorption to create chamber images and doppler
technology to determine rate and direction of
blood flow
Transducer
2
Echocardiogram
3
Stress Echocardiogram
End Systolic Resting
End Diastolic Resting
End Diastolic Max Ex
End Systolic Max Ex
4
Echocardiogram Apical 4 Chamber view
5
Septum
Apex of Heart
Apex of Heart
Papillary Muscle
RV
LV
AV
TV
MV
RA
LA
Tricuspid valve
Aortic valve
Mitral Valve
Right Atrium
Interatrial Septum
Left Atrium
Apical 4 Chamber View
6
Transesophageal Echocardiagraphy
- Advantages of TEE
- Lung air does not attenuate the sound beam
- Works better with COPD patients
- May be use during surgery
- Better visualizes
- Mitral valve disease
- Clots or other masses in the heart
- Tears in the aorta
- Prosthetic heart valves
7
Nuclear Stress Test Images
Exercise
Normal Test
Rest
Ischemic Areas
Exercise
Abnormal Test
Re-perfused after rest (no permanent damage from
an MI)
Rest
8
Cardiac Catheterization (Angiography)
- Invented by the German physician Werner Forssmann
in 1929 - Passed a catheter into his own right atrium
through the brachial artery - Performed under local anesthesia sedation
- Guide wire catheter inserted into femoral or
brachial artery - Advanced into the aorta, left ventricle, and
coronary arteries - Aortic pressure is recorded
- Contrast medium (dye) is injected into coronary
arteries - Real-time moving blood flow images are taken with
x-ray camera - Flow through the CAs appears white against
darker background - Blockages are seen as a narrowing of the white
flow - Contrast medium (dye) is injected into left
ventricle - Real-time moving images of LV motion are taken
with x-ray camera - Injected dye appears white against a darker
background - Pressures in the 4 chambers during systole and
diastole - Wall structure and motion
- ESV, EDV, SV, EF
- Heart valve function and pressure gradients
across valves
9
Left Heart Catheterization
Catheter Entering The LV and LAD Artery Via The
Aorta
- Catheter in femoral artery
- Termed left heart catheterization
- Aorta, Aortic pressures
- CA blockages
- Left ventricular function
- LVEDP LVESP
- EF
- ESV
- EDV
10
Right Heart Catheterization
Catheter Entering The RA, RV, and Pulmonary
Artery via the SuperiorVena Cava
- Catheter in subclavian or neck vein
- Termed right heart catheterization
- Pulmonary artery pressures
- Pulmonary hypertension
- Right atrial pressure
- Pulmonary capillary wedge pressure
- Same as left atrial pressure
- TC valve assessments
- Pressure gradients, etc.
11
Cardiac Catheterization Lab As Viewed Through The
Control Room
Need for emergency CABG during
PTCA 1992 1.5 2000 .014
12
LAD Catheterization Video
13
Ventriculogram (LV function)
Courtesy J. Wade Womack
14
Cath Images
LAD blockage
RCA blockage
15
Cath Images
Left Internal Carotid Artery
Blockage
Left External Carotid Artery
Left Common Carotid Artery
16
Cardiac Catheterization (Angiography)
- Risks and Possible Complications
- Bleeding around the point of incision
- Abnormal heartbeats (arrhythmias)
- Allergic reaction to the dye
- Infection
- Blood clots (stroke or pulmonary embolism)
- Perforation or other damage to the arteries
- Heart attack
- Stroke
- Air embolism
- Death (Mortality about .08)
17
Angioplasty
- PTCA Percutaneous Transluminal Coronary
Angioplasty - Currently used as primary intervention for Acute
Coronary Syndrome (MI) - Local anesthesia and sedation
- Catheter with balloon placed at the end is
advanced into blocked artery - Balloon is inflated, pressing plaque against
artery walls - Arterial lumen is increased facilitating better
blood flow. - Stent is often placed to act as scaffold to hold
artery open - Stents metal mesh sleeves that prop artery
open - Stents are sometimes coated with drugs that
inhibit re-stenosis - The site of the stent placement may receive a
dose of radiation - Called brachytherapy
- Prevents cell overgrowth in area of stent
placement - Glycoprotein IIb/IIIa inhibitors may be used to
prevent clots during placement - Plavix and aspirin are usually used to help
prevent clots post-surgery - Results are usually only temporary 18 - 40
chance of re-stenosis - Blockage almost always requires further
treatment (PTCA or CABG)
18
Angioplasty vs. Throbolytic Therapy
- Angioplasty is the most common effective
treatment for acute MI - Better results than thrombolytic (fibrinolytic)
therapy (ThT) - The use of Streptokinase, TPA, other agents to
dissolve occlusion - PTCA may be used in combination with ThT
- Stabilize patient, give ThT, PTCA done 12 to 48
hr afterwards - PTCA has d mortality rate, fewer re-infarctions,
fewer strokes - ThT should be done lt 12 hours after symptoms
- PTCA should be done lt 2 hours after arrival at
hospital - Benefits from both ThT and PTCA decline after
time windows - Bottom Linethe earlier the better for both
interventions - Use of stents for acute MI angioplasty seems to
improve outcomes - Stents associated with a 19 d in re-infarction
or repeat PTCAs
19
Mortality rate for PTCA vs Thrombolytic Therapy
in Acute MI
Mortality
N 395 395 103 1138
3145 20,683 2606
20
Outcomes for PTCA with Stent vs. PTCA only
Percent
Mortality
Reocclusion
Emergency CABG
Revascularization of same vessel
Non-fatal MI
Any Event
21
Coronary Stents
22
Blade Atherectomy
23
Rotary Atherectomy
Laser Atherectomy
24
Stent Placement
Before Stent Placement
After Stent Placement
Courtesy J. Wade Womack
25
Coronary Artery Bypass Graft Surgery (CABG)
- First modern day technique CABG performed in
1962 by Sabiston - World most expensive Plumbing Job
- Approximately 45,000 (Sollano 2002)
- General anesthesia, patients chest opened,
sternum sawed, ribs spread - Patient is placed on a respirator (ventilation
machine or ventilator) - Patients heart is stopped by perfusing the heart
with potassium - Person is placed on heart lung apparatus
- Device circulates and oxygenates blood while
heart is stopped - Cooling the heart d need for O2
- Blood be cooled while passing through heart-lung
machine - Cold saline may be poured over the heart during
surgery - Grafts harvested saphenous veins, mammarian
artery - Grafts sutured from aorta to CA, bypassing the
blockage - Takes 3 6 hours
- After surgery, patient is taken to ICU (CCU)
where he is weaned off ventilator - IVs and drainage tubes removed over the next 48
hours (longer in older people) - Patients eating on their own after 24 hours and
rehab is begun within 48 hours - Patients with no complications go home after
about 4 days
26
(No Transcript)
27
Modern Heart Lung Machine
First Heart Lung Machine developed in 1953 and
used in the surgical closure an atrial defect in
an 18 year old girl
28
CABG Surgery
Rib Spreader Reveals Heart
Graft be anastamosed (sutured) to CA
29
Coronary Artery Bypass Graft Surgery (CABG)
- Risks and Possible Complications
- Risks associated with anesthesia
- respiratory failure
- Bleeding
- Abnormal heartbeats (arrhythmias A-fib /
A-flutter is common) - may need pacemaker
- Infection at incision sites
- Blood clots and plaque (stroke or PE, blocking
of O2 to tissues) - Memory loss and problems with cognitive function
- Heart attack
- Pneumonia
- Hypotension from being on heart-lung machine r
Kidney failure - Heart failure
- Swelling of ankles or feet on the leg where graft
was removed - Depression, anxiety and other emotional
difficulties - Post Pump Syndrome
- systemic inflamation in lungs r edema, kidneys r
kidney failure - Death (Mortality about 1.5..15 for redos)
30
Notes on CABG surgery
- CABG is usually not the first consideration for
treatment - not done unless the risks of not having the
procedure are high - 50 of grafts develop lesions within 10 years
- Rate may be reduced by statin drugs
- 516,000 CABG surgeries done every year
- Routine surgery today
- Very high success rate (97- 99)
- 67 of patients report NO COMPLICATIONS
31
Recent Developments In Cardiac Surgery
- Off-Pump Coronary Artery Bypass (OPCAB)
- Same as regular CABG but with no heart lung
machine - Drugs such as Adenosine and Esmolol are used to
slow HR - Could be performed 30 - 40 of the time when
CABG surgery is needed - Minimally Invasive Direct Coronary Artery Bypass
(MIDCAB) - Smaller transverse incision
- No sternotomy, done on beating heart (drugs used
to slow HR) - Use of radial artery for grafts (grafts last
longer) - Gene therapy (inhibits hyperplasia of intimal
cells) - Transmyocardial Laser Revascularization (TMLR)
- Lasing holes directly into myocardium to u
myocardial blood supply - Based on reptile heart which has no CAs
- Stem cells injected into myocardium of CHF
patients - Increase myocardial tissue or form new
vasculature? - Stem cells injected into CAs during
revascularization - Mixed results some arteries re-stenosed at a
higher rate
Recommended
CrystalGraphics Presentations





























