
Genital Tuberculosis - PowerPoint PPT Presentation
1 / 74
Title:
Genital Tuberculosis
Description:
Management of Infertility in Genital Tuberculosis? Answer Tubal reconstructive surgery is contraindicated because there is usually irreparable damage of tubes (cilia ... – PowerPoint PPT presentation
Number of Views:6650
Avg rating:3.0/5.0
Title: Genital Tuberculosis
1
Genital Tuberculosis
2
- Dr Ajit Virkud
- Professor, and Head of Department,
- K.B.B.Hospital, Bandra, Mumbai.
- Consultant,
- Bhatia Hospital, Mumbai
3
Who said this?
THERE IS A DREAD DISEASE.. IN WHICH LIFE AND
DEATH ARE SO STRONGLY BLENDED THAT DEATH TAKES
THE GLOW AND HUE OF LIFE, AND LIFE THE GAUNT AND
GRISLY FORM OF DEATH.
- What was he referring to?
4
Answer
- Charles Dickens referring to Tuberculosis
5
Who discovered the Tubercle Bacillus?
6
Answer
- Robert Koch discovered the tubercle bacilli in
1882. - The word tuberculosis was first used in 1834.
7
What was this disease called in ancient Indian
Vedas?
8
Answer
- Tuberculosis was known as Raksyasman - king of
diseases, in the ancient Indian Vedas
9
Who described the first case of genital TB?
- Who described the first case of TB endometritis?
10
Answer
- First recorded case of genital tuberculosis was
described by Morgagni in 1744 - First case of tubercular endometritis was
reported by Kiwsch in 1847.
11
Which country has the highest incidence of TB?
12
Answer
- India has the highest incidence in the world. The
reported incidence in India is 2-10 (Malkani,
1975 9.3, Agarwal, 1993 2.4).
13
What is Mycobacterium tuberculosis complex?
- MTB complex?
14
Answer
- It comprises
- M. tuberculosis hominis
- M. bovis
- M. africanum (atypical Mycobacteria spp.)
- Tuberculosis in humans is mainly caused by
bacteria called M. tuberculosis hominis
(occasionally mycobacterium bovis or atypical
tuberculosis organisms are also found).
15
How does TB bacillus differ from other bacteria?
- Why does it not respond to commonly used
anti-bacterial agents?
16
Answer
- Tuberculosis organism is a non-motile obligate
aerobe with replicating cycle of 17-24 hours
(slow growing) - It does not have a capsule.
- It has a property of being acid-fast due to the
surface lipids. This property makes it resistant
to common antibacterial agents and lytic enzymes.
17
How does Tuberculosis spread?
- Is it a sexually transmitted disease?
18
Answer
- Hematogenous spread according to Magnus Hames
this is the commonest mode of spread seen in 90
of cases. - Descending infection (7) direct or lymphatic
spread from the peritoneum, bowel or mesenteric
lymph nodes - Ascending infection rarely (1-2 cases)
infection occurs from coitus with a male
suffering from urogenital tuberculosis or by use
of infected sputum as a lubricant for intercourse
or in children who sit naked on infected sputum.
19
On PV examination F. Tubs are palpable?
- What is your diagnosis?
20
Answer
- Thickened, palpable fallopian tubes suggests
tubercular salpingitis.
21
What is frozen pelvis?
- What is its differential diagnosis?
22
Answer
- When all pelvic structures are matted together
and fixed with the uterus it results in frozen
pelvis. - DD of frozen pelvis?
- Florid genital tuberculosis
- Grade III/IV pelvic endometriosis
- Advance invasive carcinoma of cervix
- Following radiotherapy for invasive carcinoma of
cervix
23
You are doing D C to rule out TB endometritis.
- How do you obtain the endometrium and how do you
send the sample?
24
Answer
- One must do a thorough curettage, including bothy
cornual regions (common sites for TB
endometritis) - Entire endometrium is collected and divided in
two parts - Half in for formalin for histopathological
examination to look for tuberculous granulomas. - Other half in saline for smear / culture / guinea
pig inoculation. Smear Ziehl Neelson stain
25
How do you obtain a sample in adolescent
unmarried girls?
- In virginal adolescent girls with s/s of PID one
must rule out Genital TB.
26
Answer
- In unmarried adolescent girls menstrual discharge
collected within 12 hours of onset of menses can
be used for culture.
27
What are the different culture media used for TB?
28
Answer
- Various culture media used are
- Lowenstein Jensen medium (color malachite green),
- Dorset's egg, Petroff's,
- Tween 80, Dubois medium
- Colonies are cream colored, raised, coarsely
granular dry friable and rough with spreading
edges suggests virulent forms. - Culture report takes 3-6 weeks.
29
Is Guinea pig inoculation essential for diagnosis?
- Can you use any other animal for testing?
30
Answer
- Animal inoculation is the only investigation
accepted as confirmatory evidence of TB Smaller
lab animals like mice can be used
31
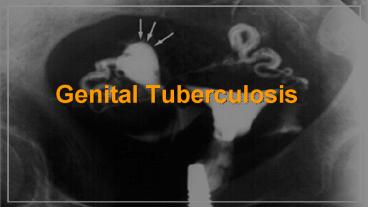
Read this HSG
- What is your diagnosis?
32
Answer
- HSG showing sperm head appearance suggesting TB
salpingitis.
33
Read this hsg?
- What is your diagnosis?
34
Answer
- Moth eaten appearance suggestive of TB
endometritis
35
Read this HSG?
- What is your diagnosis?
36
Answer
- Venous Lymphatic Intravasation
- DD
- Genital TB
- False passage
- Hsg done during or just after menses
- Injection of dye in a patient with bilateral
cornual block
37
Read this HSG?
- What is your diagnosis?
38
Answer
- Tobacco Pouch Appearance seen in genital TB
39
What are the HSG findings suggestive of pelvic
tuberculosis ?
40
Answer In F. Tubes
- Bilateral blocked tubes especially at cornual end
- Beaded appearance
- Irregular shaggy outline of tubes
- Golf club/ sperm head appearance small
sacculation at the filling end of
isthmus/ampullary portion of tube - Maltese cross appearance in fibrotic
stage-curved or straight pipe-like appearance of
tubes with lack of normal tortuosity - Multiple filling defects, diverticuli or
extravasation in tubal wall
41
Answer In F. Tubes
- Leopard skin appearance the ampulla of the tube
is partially filled with dye giving a speckled
appearance - Rosette the distal end of the tube is filled
with dye that has a rosette appearance - Tobacco pouch appearance
- Straight thickened, rigid pipe stem tubes
- Hydrosalpinx/ pyosalpinx
- Calcification in tubes
42
Answer In Uterus
- Moth-eaten appearance irregular outline of
cavity (TB endometritis) - Intra-uterine adhesions (synichae)
- Venous/lymphatic intravasation of dye
43
What is Blue Uterus Sign?
- What is the role of laparoscopy in diagnosis of
genital TB?
44
Answer
Laparoscopy should be done carefully to avoid
injury to adherent bowel loops open laparoscopy
is preferred.
- Blue uterus when chromopertubation test done
with methylene blue - Acute salpingitis red, swollen edematous tubes
- Tiny tubercles 1-4 mm on surface of organs
tubes, uterus - Hydrosalpinx, pyosalpinx
- Tobacco-pouch appearance
- Violin string adhesions
- Unilateral / bilateral TO masses
- Straw colored thick jelly like exudate in POD
- Fimbrial biopsy, peritoneal fluid may be taken to
confirm the diagnosis
45
What are the usg findings suggestive of TB?
46
Answer
- Loculated ascites The presence of fine lacy
strands or particulate matter in fluid is due to
thin fibrin strands - Bilateral or unilateral tubo-ovarian mass
47
What is Mitchison Grosset Hypothesis
- What was he referring to?
48
Answer
Group I Fast growing, neutral pH, aerobic
Group II Slow growing, intracellular, acidic
Group III Slow growing, neutral pH, hypoxic
Dormant bacilli
THE BATTLE AGAINST TUBERCULOSIS CANNOT BE WON
UNTIL DRUGS THAT CAN EFFECTIVELY KILL THESE
DORMANT TUBERCULOUS BACILLI ARE FOUND.
49
Which drugs are used in the 4 drug short course
treatment?
- Why are these drugs used?
50
Answer
Drug Bactericidal activity
Isoniazide Bactericidal in-vivo and in-vitro
Rifampicin Bactericidal in-vivo and in-vitro
Pyrazinamide Selectively bactericidal
Streptomycin Selectively bactericidal
51
What are the doses of these 4 drugs?
- Can you give these drugs twice weekly? On what
basis?
52
Answer
Drug Dose (lt50 Kg) Dose (gt50 Kg) Twice wkly dose
Isoniazid (Z) 300 mg 450mg (8-12mg / Kg 600-900 mg
Rifampicin (R) 450 mg 600 mg Tab. 600 mg
Pyrazinamide (Z) 1500 mg 2000 mg 3000 mg
Ethambutol (E) 1200 mg 1500 mg 2400 mg
THE REASON WHY ANTI-TUBERCULOUS DRUGS CAN BE
EFFECTIVELY GIVEN IN TWICE WEEKLY DOSES ALSO IS
BECAUSE M. TUBERCULOSIS IS A SLOW GROWING
ORGANISM (REPLICATING CYCLE OF 17-24 HOURS).
53
What is DOTS?
54
Answer
- WHO declared tuberculosis a global emergency in
1993. World health assembly (WHA) set two
targets for TB control to be reached by 2000 - Detection of 70 of all new sputum-smear positive
cases arising each year - Treat 85 of these cases successfully
- To achieve this WHO promoted a new effective TB
control program based on five essential elements
called the Directly Observed Treatment Short
course (DOTS) strategy
55
Answer The five elements are
- Continued political commitment from governments
- Case detection through quality-assured
bacteriology - Standardized short-course chemotherapy (mentioned
in detail below) for 6-8 months involving
directly observing the patient - An effective drug supply and management system
- Monitoring and evaluation system for overall
assessment of program performance.
56
Answer
- It is defined as supervised intake of drugs five
times a week for 8 weeks (in India, the patient
is observed to take the drug daily in the
intensive phase) and then three times a week for
4 months. - The patients are given fixed drug combipack.
- The observer should be accessible, acceptable and
accountable.
57
What is DOTS plus strategy?
58
Answer
- Patients who have a relapse or failure are
categorized into WHO category II. - In the initial phase they are given intramuscular
injections of streptomycin thrice weekly for two
months along with four drugs of category I (RHZE)
under direct supervision. This is followed by
four drugs (RHZE) thrice a week for another
month. In the continuation phase they are given
three drugs (RHE) thrice a week for 5 more months
under direct observation.
59
What is MDR XDR TB?
60
Answer
- Resistance to one drug e.g. rifampicin or
isoniazid is called drug resistant tuberculosis.
Resistance to both main anti-tuberculous drugs is
called multi-drug resistance (MDR) whereas
resistance to many drugs namely isoniazid,
rifampicin, injectable amino-glycosides and
fluroquinolones is called extreme drug
resistance (XDR). - Drug resistant tuberculosis is treated as
category IV with a DOTS Plus strategy
61
Answer
- Drug resistant tuberculosis is treated as
category IV with a DOTS Plus strategy comprising
six second line drugs daily for six months
followed by four drugs for the next 18 months in
the continuation phase.
62
What are the reserve line of drugs used in
treatment of TB?
63
Answer
Drug lt50 Kg gt50 Kg
Thiacetazone 150 mg 150 mg
Ethionamide 500 mg 750 mg
Cyclocerine 750 mg 1000 mg
Inj. Kanamycin 750 mg 1000 mg
Inj. Capreomycin 750 mg 1000 mg
Inj. Viomycin 750 mg 1000 mg
64
What are the newer drugs used in the treatment of
drug resistant TB?
65
Answer
- Fluoroquinolones Ciprofloxacin (1500 mg/day),
and Ofloxacin (400-600 mg/day) for 6 months - Anti-leprosy drugs Clofazine (100-200 mg/day)
- Beta-lactam antibiotics amoxicillin clavulanic
acid (Augmentin) - Macrolides azithromycin, roxithromycin, and
clarithromycin
66
Management of Infertility in Genital Tuberculosis?
67
Answer
- Tubal reconstructive surgery is contraindicated
because there is usually irreparable damage of
tubes (cilia are destroyed) - May result in reactivation and dissemination
- Those with infertility must be treated with
medical treatment and if this does not help
artificial reproductive techniques may be
considered. However one must remember that in the
presence of TB endometritis, the results of
embryo transfer are disappointing.
68
What is the role of surgery in treatment of
genital TB?
69
Answer
- Only surgical treatment possible is extirpative
surgery with bilateral salpingo-oophorectomy - Anti-TB chemotherpy started 2 weeks prior and
continued for 6 months post-operatively. - Indications for TAH with BSO are
- Failure of medical line of treatment progression
or persistence of active tuberculosis - Large T-O masses, pyosalpinx, pyometra or ovarian
abscess in a symptomatic patient of
perimenopausal age group.
70
Answer
- Contraindications to surgery
- Active tuberculosis elsewhere in body
- Plastic peritonitis or dense adhesions around
pelvic organs. - During surgery do not use non-absorbable sutures
because of risk of fistula / sinus - Vulvectomy may be required in cases of
hypertrophic vulvar involvement.
71
What is the prognosis in genital TB cases as
regards fertility?
72
Answer
- Prognosis for child-bearing is very poor almost
nil if endometrium is destroyed. - Only 2-5 patients will conceive
- 20-30 will have spontaneous abortion
- 40-50 ectopic pregnancy
- Only 20 will go to full term
- Even after ART, the prognosis is poor especially
if endometrium is destroyed
73
If mankind is to win the war against tuberculous
organism, it is imperative that world bodies like
WHO, Stop TB Organization and TB Alliance should
work together to develop new and effective
anti-tuberculous drugs and vaccines.
- Tuberculosis Minded
74
- Thank You!
Recommended
CrystalGraphics Presentations





























